

Gaps in the implementation of antenatal syphilis detection and treatment in health facilities across sub-Saharan Africa
- PMID: 29856849
- PMCID: PMC5983468
- DOI: 10.1371/journal.pone.0198622
Gaps in the implementation of antenatal syphilis detection and treatment in health facilities across sub-Saharan Africa
Abstract
Background: Syphilis in pregnancy is an under-recognized public health problem, especially in sub-Saharan Africa which accounts for over 60% of the global burden of syphilis. If left untreated, more than half of maternal syphilis cases will result in adverse pregnancy outcomes including stillbirth and fetal loss, neonatal death, prematurity or low birth weight, and neonatal infections. Achieving universal coverage of antenatal syphilis screening and treatment has been the focus of the global campaign for the elimination of mother-to-child transmission of syphilis. However, little is known about the availability of antenatal syphilis screening and treatment across sub-Saharan Africa. The objective of this study was to estimate the 'likelihood of appropriate care' for antenatal syphilis screening and treatment by analyzing health facility surveys and household surveys conducted from 2010 to 2015 in 12 sub-Saharan African countries.
Methods: In this secondary data analysis, we linked indicators of health facility readiness to provide antenatal syphilis detection and treatment from Service Provision Assessments (SPAs) and Service Availability and Readiness Assessments (SARAs) to indicators of ANC use from the Demographic and Health Surveys (DHS) to compute estimates of the 'likelihood of appropriate care'.
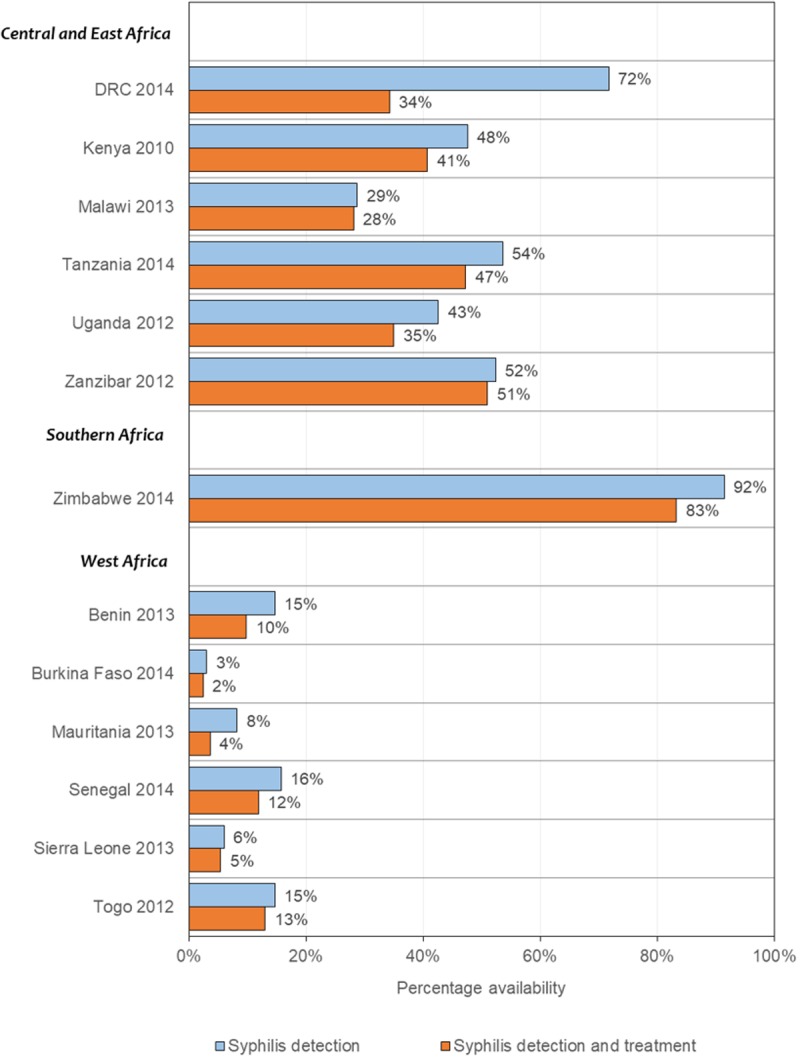
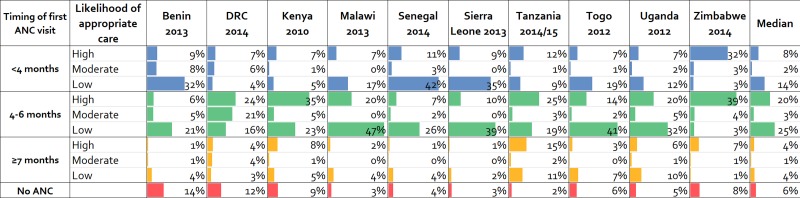
Results: Based on data from 5,593 health facilities that reported offering antenatal care (ANC) services, the availability of syphilis detection and treatment in ANC facilities ranged from 2% to 83%. The availability of syphilis detection and treatment was substantially lower in ANC facilities in West Africa compared to the other sub-regions. Levels of ANC attendance were high (median 94.9%), but only 27% of ANC attendees initiated care at less than 4 months gestation. We estimated that about one in twelve pregnant women received ANC early (<4 months) at a facility ready to provide syphilis detection and treatment (median 8%, range 7-32%). The largest implementation bottleneck identified was low health facility readiness, followed by timeliness of the first ANC visit.
Conclusions: While access was fairly high, the low levels of likelihood of antenatal syphilis detection and treatment identified reinforce the need to improve the availability of syphilis rapid diagnostic tests and treatment and the timeliness of antenatal care-seeking across sub-Saharan Africa.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Gomez GB, Kamb ML, Newman LM, Mark J, Broutet N, Hawkes SJ. Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ. 2013;91:217–26. doi: 10.2471/BLT.12.107623 - DOI - PMC - PubMed
-
- Ward H, Ronn M. Contribution of sexually transmitted infections to the sexual transmission of HIV. Curr Opin HIV AIDS. 2010. July;5(4):305–10. doi: 10.1097/COH.0b013e32833a8844 - DOI - PMC - PubMed
-
- Mwapasa V, Rogerson SJ, Kwiek JJ, Wilson PE, Milner D, Molyneux ME, et al. Maternal syphilis infection is associated with increased risk of mother-to-child transmission of HIV in Malawi. AIDS. 2006;20(14). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
