

Efficacy and safety of fluticasone propionate/formoterol fumarate in pediatric asthma patients: a randomized controlled trial
- PMID: 29857783
- PMCID: PMC5985608
- DOI: 10.1177/1753466618777924
Efficacy and safety of fluticasone propionate/formoterol fumarate in pediatric asthma patients: a randomized controlled trial
Abstract
Background: The efficacy and safety of fluticasone propionate/formoterol fumarate pressurized metered-dose inhaler (pMDI) (fluticasone/formoterol; Flutiform®; 100/10 µg b.i.d.) was compared with fluticasone propionate (Flixotide® Evohaler® pMDI; 100 µg b.i.d.) and fluticasone/salmeterol (Seretide® Evohaler® pMDI; 100/50 µg b.i.d.) in a pediatric asthma population (EudraCT number: 2010-024635-16).
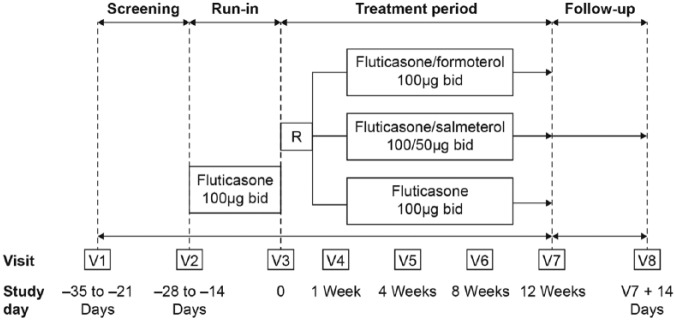
Methods: A double-blind, double-dummy, parallel group, multicenter study. Patients, aged 5-<12 years with persistent asthma ⩾ 6 months and forced expiratory volume in 1 s (FEV1) ⩽ 90% predicted were randomized 1:1:1 to 12 weeks' treatment. The study objectives were to demonstrate superiority of fluticasone/formoterol to fluticasone and non-inferiority to fluticasone/salmeterol.
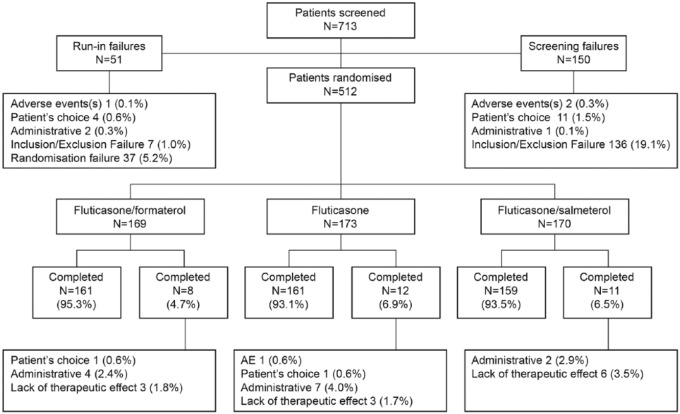
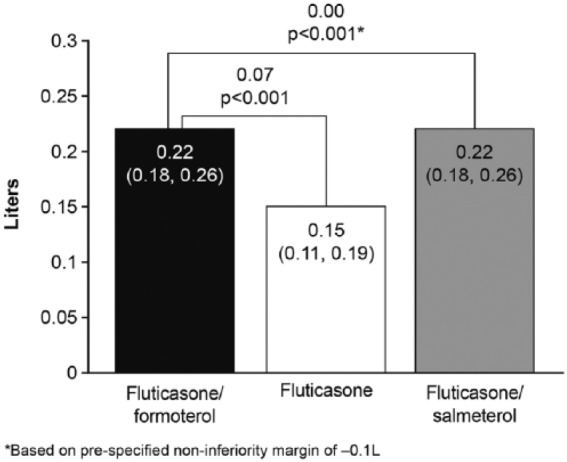
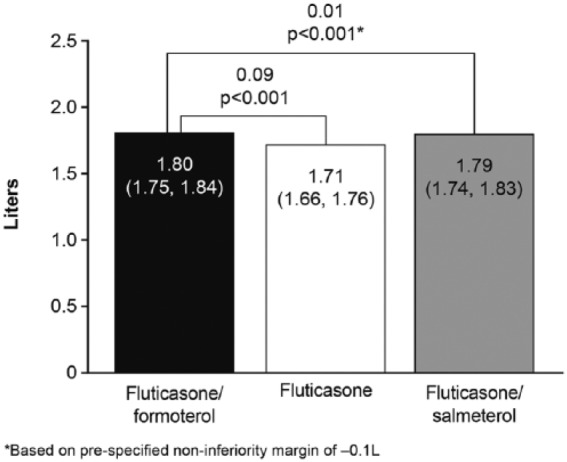
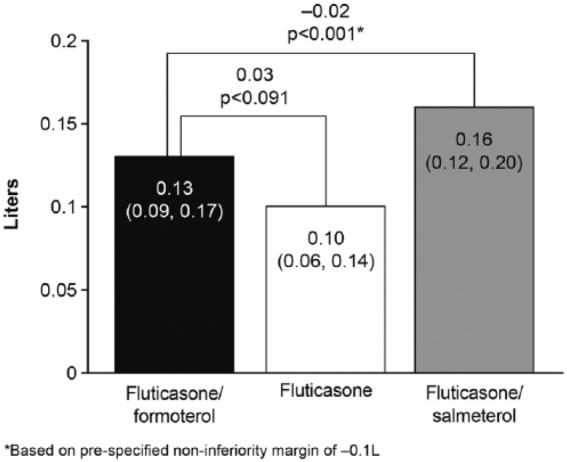
Results: A total of 512 patients were randomized: fluticasone/formoterol, 169; fluticasone, 173; fluticasone/salmeterol, 170. Fluticasone/formoterol was superior to fluticasone for the primary endpoint: change from predose FEV1 at baseline to 2 h postdose FEV1 over 12 weeks [least squares (LS) mean difference 0.07 l; 95% confidence interval (CI) 0.03, 0.11; p < 0.001] and the first key secondary endpoint, FEV1 area under the curve over 4 hours (AUC0-4 h) at week 12 (LS mean difference 0.09 l; 95% CI: 0.04, 0.13; p < 0.001). Per a prespecified non-inferiority margin of -0.1 l, fluticasone/formoterol was non-inferior to fluticasone/salmeterol for the primary endpoint (LS mean difference 0.00 l; 95% CI -0.04, 0.04; p < 0.001) and first key secondary endpoint (LS mean difference 0.01; 95% CI -0.03, 0.06; p < 0.001). Fluticasone/formoterol was non-inferior to fluticasone/salmeterol for the second key secondary endpoint, change from predose FEV1 over 12 weeks (treatment difference -0.02 l; 95% CI -0.06, 0.02; p < 0.001), but was not superior to fluticasone for this endpoint (LS mean difference 0.03 l; 95% CI -0.01, 0.07; p = 0.091). All treatments elicited large improvements from baseline to week 12 for the Pediatric Asthma Quality of Life Questionnaire (LS mean change 0.76 to 0.85 units) and Asthma Control Questionnaire (LS mean change -1.03 to -1.13 units). Few severe exacerbations were seen (fluticasone/formoterol: two; fluticasone/salmeterol: two). All treatments were well tolerated.
Conclusions: This study supports the efficacy and safety of fluticasone/formoterol in a pediatric asthma population and its superiority to fluticasone.
Keywords: ICS/LABA; asthma; children; combination therapy; fluticasone propionate; formoterol fumarate.
Conflict of interest statement
Anna Ploszczuk and Miroslava Bosheva have no conflicts of interest to disclose.
Figures
References
-
- Global Initiative for Asthma. GINA Global Strategy for Asthma Management and Prevention, 2016; http://ginasthma.org/
-
- GlaxoSmithKline Briefing Document. Benefit risk assessment of salmeterol for the treatment of asthma in adults and children, 2008; https://wayback.archive-it.org/7993/20170405035641/https://www.fda.gov/ohrms/dockets/ac/08/briefing/2008-4398b1-04-GSK.pdf
-
- Bodzenta-Lukaszyk A, Pulka G, Dymek A, et al. Efficacy and safety of fluticasone and formoterol in a single pressurized metered dose inhaler. Respir Med 2011; 105: 674–682. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
