

Diabetes and Trajectories of Estimated Glomerular Filtration Rate: A Prospective Cohort Analysis of the Atherosclerosis Risk in Communities Study
- PMID: 29858211
- PMCID: PMC6054502
- DOI: 10.2337/dc18-0277
Diabetes and Trajectories of Estimated Glomerular Filtration Rate: A Prospective Cohort Analysis of the Atherosclerosis Risk in Communities Study
Abstract
Objective: To characterize long-term kidney disease trajectories in persons with and without diabetes in a general population.
Research design and methods: We classified 15,517 participants in the community-based Atherosclerosis Risk in Communities (ARIC) study by diabetes status at baseline (1987-1989; no diabetes, undiagnosed diabetes, and diagnosed diabetes). We used linear mixed models with random intercepts and slopes to quantify estimated glomerular filtration rate (eGFR) trajectories at four visits over 26 years.
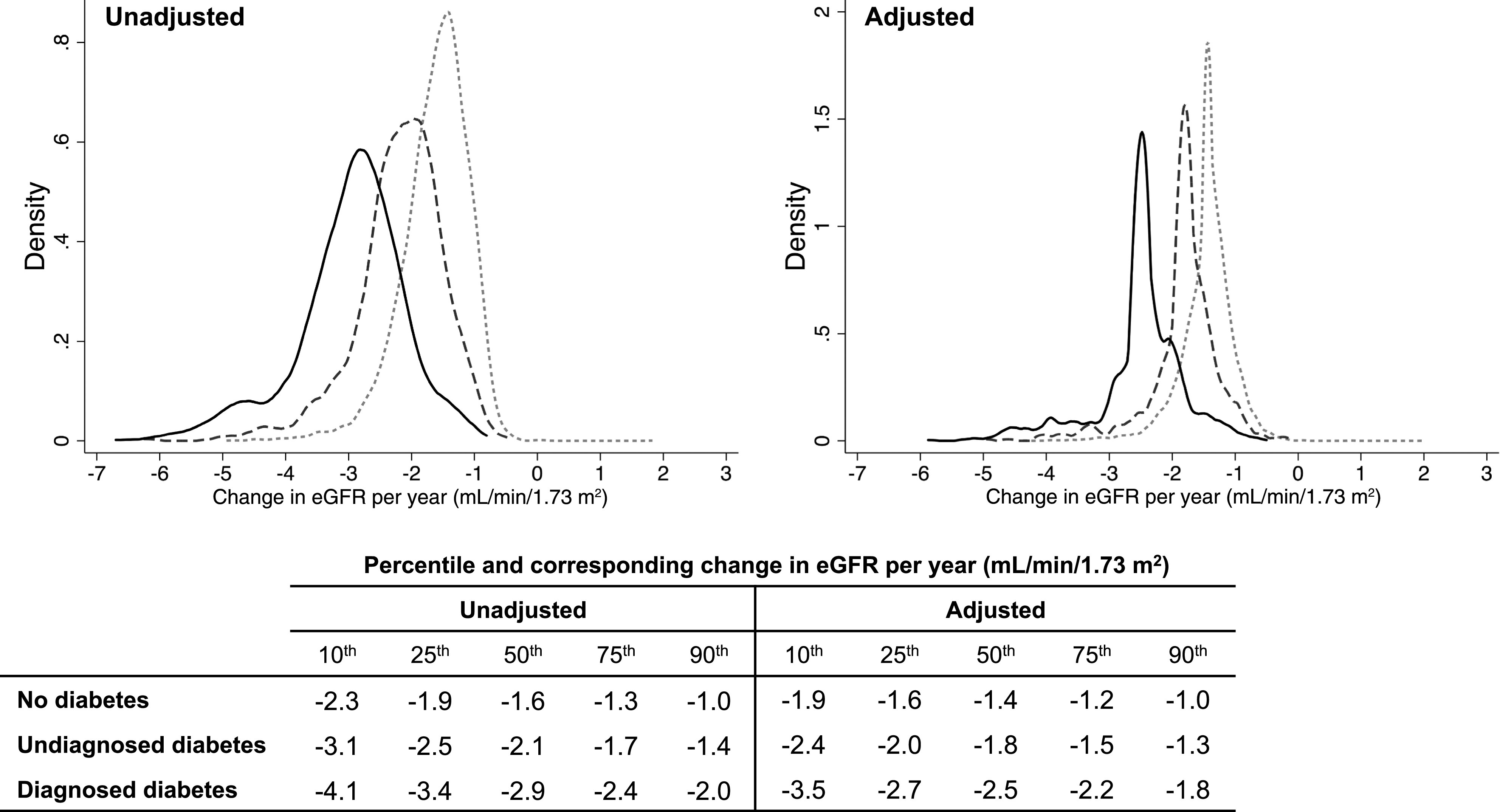
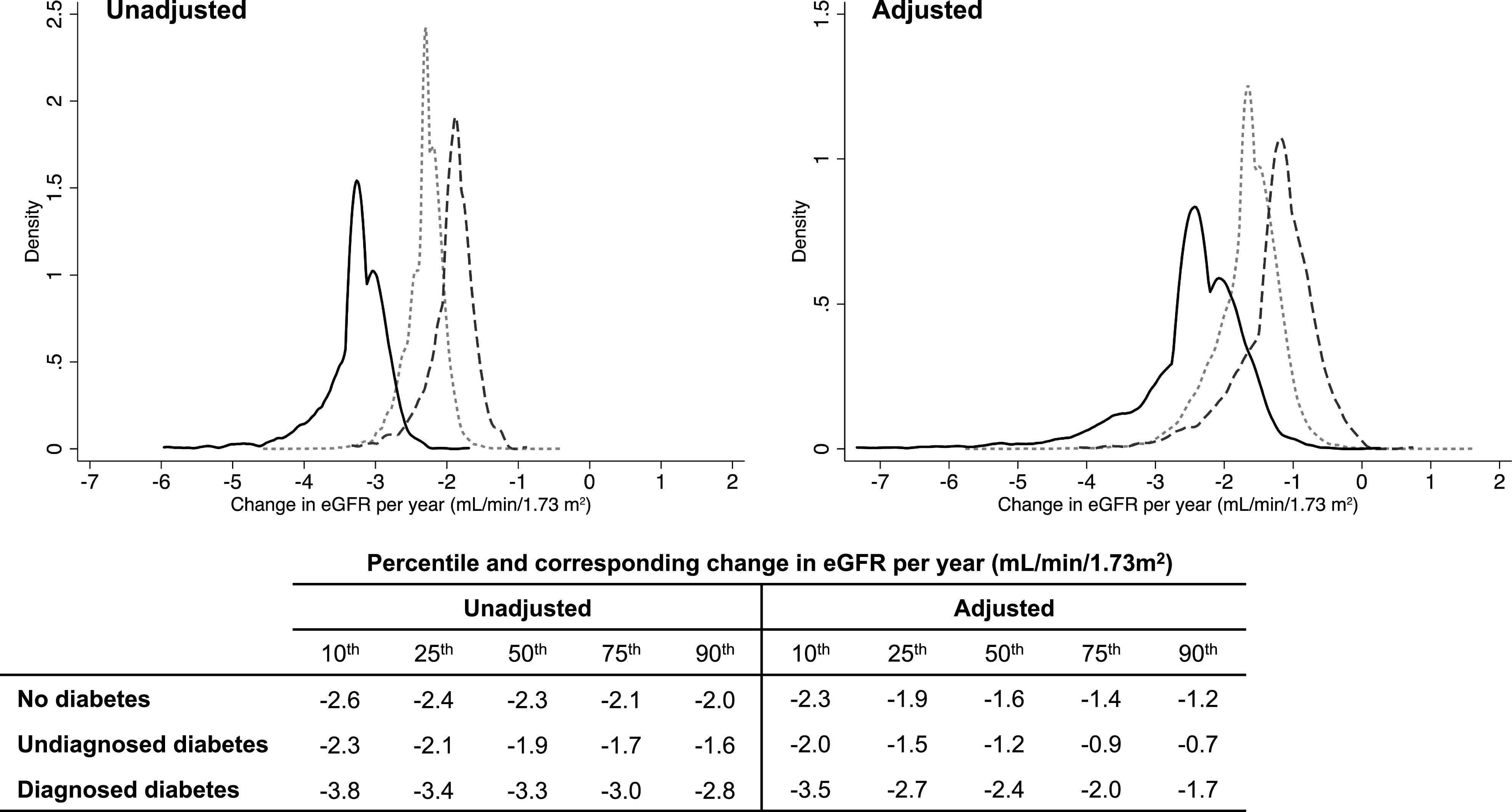
Results: Adjusted mean eGFR decline over the full study period among participants without diabetes was -1.4 mL/min/1.73 m2/year (95% CI -1.5 to -1.4), with undiagnosed diabetes was -1.8 mL/min/1.73 m2/year (95% CI -2.0 to -1.7) (difference vs. no diabetes, P < 0.001), and with diagnosed diabetes was -2.5 mL/min/1.73 m2/year (95% CI -2.6 to -2.4) (difference vs. no diabetes, P < 0.001). Among participants with diagnosed diabetes, risk factors for steeper eGFR decline included African American race, APOL1 high-risk genotype, systolic blood pressure ≥140 mmHg, insulin use, and higher HbA1c.
Conclusions: Diabetes is an important risk factor for kidney function decline. Those with diagnosed diabetes declined almost twice as rapidly as those without diabetes. Among people with diagnosed diabetes, steeper declines were seen in those with modifiable risk factors, including hypertension and glycemic control, suggesting areas for continued targeting in kidney disease prevention.
© 2018 by the American Diabetes Association.
Figures
Comment in
-
Comment on Warren et al. Diabetes and Trajectories of Estimated Glomerular Filtration Rate: A Prospective Cohort Analysis of the Atherosclerosis Risk in Communities Study. Diabetes Care 2018;41:1646-1653.Diabetes Care. 2019 Mar;42(3):e51-e52. doi: 10.2337/dc18-2288. Diabetes Care. 2019. PMID: 30787065 No abstract available.
References
-
- Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA 2015;314:1021–1029 - PubMed
-
- United States Renal Data System 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2017
-
- Levey AS, Inker LA, Matsushita K, et al. . GFR decline as an end point for clinical trials in CKD: a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am J Kidney Dis 2014;64:821–835 - PubMed
-
- Poretsky L. (Ed.). Principles of Diabetes Mellitus. 3rd ed New York, Springer International Publishing, 2017
Publication types
MeSH terms
Grants and funding
- R01 DK089174/DK/NIDDK NIH HHS/United States
- K01 DK107782/DK/NIDDK NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- K08 DK092287/DK/NIDDK NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
