

Barriers to effective diabetes management - a survey of people with severe mental illness
- PMID: 29859061
- PMCID: PMC5984777
- DOI: 10.1186/s12888-018-1744-5
Barriers to effective diabetes management - a survey of people with severe mental illness
Abstract
Background: People with severe mental illnesses (SMI) such as schizophrenia and bipolar disorder have an increased risk of developing type 2 diabetes and have poorer health outcomes than those with diabetes alone. To maintain good diabetes control, people with diabetes are advised to engage in several self-management behaviours. The aim of this study was to identify barriers or enablers of diabetes self-management experienced by people with SMI.
Methods: Adults with type 2 diabetes and SMI were recruited through UK National Health Service organisations and mental health and diabetes charities. Participants completed an anonymous survey consisting of: Summary of Diabetes Self-Care Activities (SDSCA); CORE-10 measure of psychological distress; a measure of barriers and enablers of diabetes self-management based on the Theoretical Domains Framework; Diabetes UK care survey on receipt of 14 essential aspects of diabetes healthcare. To identify the strongest explanatory variables of SDSCA outcomes, significant variables (p < .05) identified from univariate analyses were entered into multiple regressions.
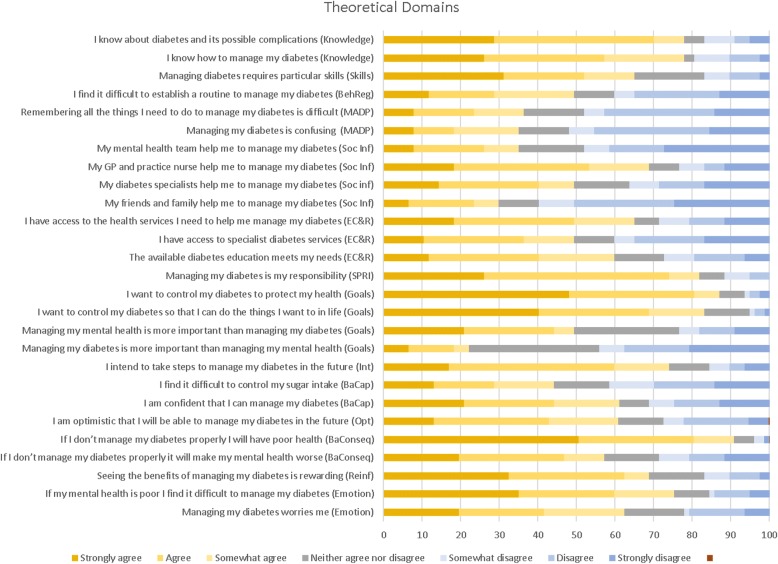
Results: Most of the 77 participants had bipolar disorder (42%) or schizophrenia (36%). They received a mean of 7.6 (SD 3.0) diabetes healthcare essentials. Only 28.6% had developed a diabetes care plan with their health professional and only 40% reported receiving specialist psychological support. Engagement in self-management activities was variable. Participants reported taking medication on 6.1 (SD 2.0) days in the previous week but other behaviours were less frequent: general diet 4.1 (2.3) days; specific diet 3.6 (1.8) days, taking exercise 2.4 (2.1) days and checking feet on 1.7 (1.8) days. Smoking prevalence was 44%. Participants reported finding regular exercise and following a healthy diet particularly difficult. Factors associated with diabetes self-management included: the level of diabetes healthcare and support received; emotional wellbeing; priority given to diabetes; perceived ability to manage diabetes or establish a routine to do so; and perceived consequences of diabetes self-management.
Conclusions: Several aspects of diabetes healthcare and self-management are suboptimal in people with SMI. There is a need to improve diabetes self-management support for this population by integrating diabetes action plans into care planning and providing adequate psychological support to help people with SMI manage their diabetes.
Keywords: Diabetes; Self-management; Service users; Severe mental illness; Theoretical domains framework.
Conflict of interest statement
Ethics approval and consent to participate
The study received ethical approval from the National Health Service (NHS) Health Research Authority Proportionate Review Sub-Committee of the National Research Ethics Service Committee Wales REC 7. REC Reference 15/WA/0310. The Committee approved the research, noting that it met the requirements of the Mental Capacity Act 2005 and confirming that it was not necessary for consultees to be appointed for potential participants. Approval was also obtained from the Primary Care Clinical Commissioning Groups and the Research and Development office of the NHS Trusts where the research was conducted. Participants provided consent by ticking a box on the electronic survey or paper questionnaire to confirm that they had read the Participant Information Sheet and agreed to take part in the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
