

Why not? Understanding the spatial clustering of private facility-based delivery and financial reasons for homebirths in Nigeria
- PMID: 29859092
- PMCID: PMC5984741
- DOI: 10.1186/s12913-018-3225-4
Why not? Understanding the spatial clustering of private facility-based delivery and financial reasons for homebirths in Nigeria
Abstract
Background: In Nigeria, the provision of public and private healthcare vary geographically, contributing to variations in one's healthcare surroundings across space. Facility-based delivery (FBD) is also spatially heterogeneous. Levels of FBD and private FBD are significantly lower for women in certain south-eastern and northern regions. The potential influence of childbirth services frequented by the community on individual's barriers to healthcare utilization is under-studied, possibly due to the lack of suitable data. Using individual-level data, we present a novel analytical approach to examine the relationship between women's reasons for homebirth and community-level, health-seeking surroundings. We aim to assess the extent to which cost or finance acts as a barrier for FBD across geographic areas with varying levels of private FBD in Nigeria.
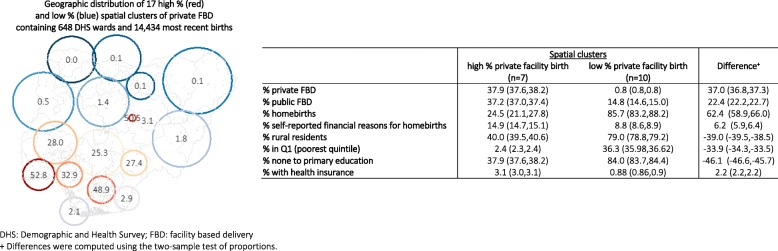
Method: The most recent live births of 20,467 women were georeferenced to 889 locations in the 2013 Nigeria Demographic and Health Survey. Using these locations as the analytical unit, spatial clusters of high/low private FBD were detected with Kulldorff statistics in the SatScan software package. We then obtained the predicted percentages of women who self-reported financial reasons for homebirth from an adjusted generalized linear model for these clusters.
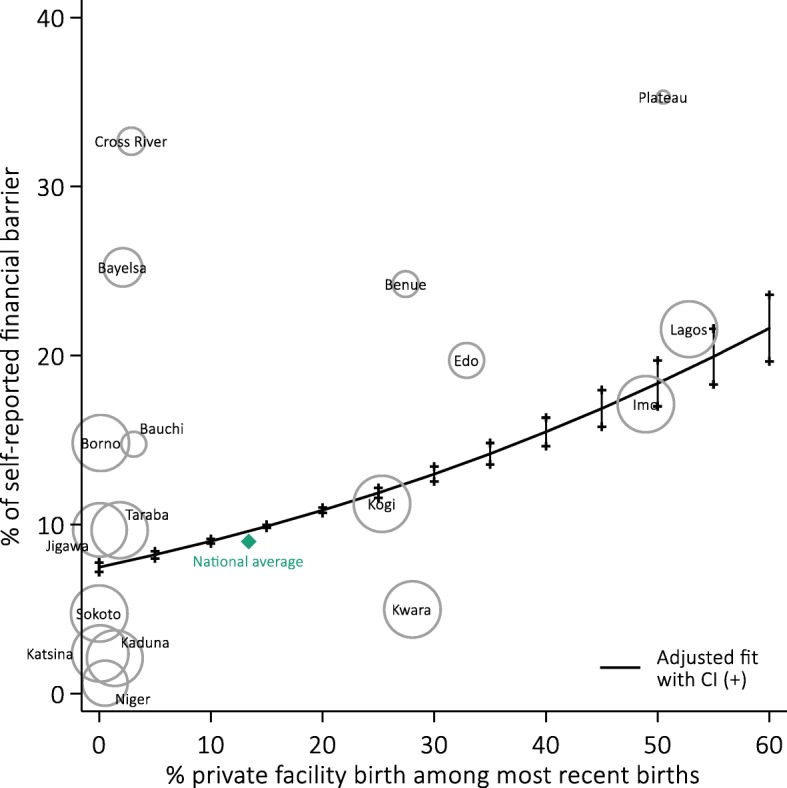
Results: Overall private FBD was 13.6% (95%CI = 11.9,15.5). We found ten clusters of low private FBD (average level: 0.8, 95%CI = 0.8,0.8) and seven clusters of high private FBD (average level: 37.9, 95%CI = 37.6,38.2). Clusters of low private FBD were primarily located in the north, and the Bayelsa and Cross River States. Financial barrier was associated with high private FBD at the cluster level - 10% increase in private FBD was associated with + 1.94% (95%CI = 1.69,2.18) in nonusers citing cost as a reason for homebirth.
Conclusions: In communities where private FBD is common, women who stay home for childbirth might have mild increased difficulties in gaining effective access to public care, or face an overriding preference to use private services, among other potential factors. The analytical approach presented in this study enables further research of the differentials in individuals' reasons for service non-uptake across varying contexts of healthcare surroundings. This will help better devise context-specific strategies to improve health service utilization in resource-scarce settings.
Keywords: Clustering; Facility childbirth delivery; Financial barrier; Maternal health service utilization; Private health services; Spatial epidemiology.
Conflict of interest statement
Ethics approval and consent to participate
The DHS receive government permission and obtain informed consent from all participants. The Research Ethics Committee of the London School of Hygiene and Tropical Medicine approved our secondary analysis of anonymised data.
Consent for publication
The consent to publish is not applicable for the current analysis as individual data is not reported.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Wekesah, F. M., Adedini, S. A. Osotimehin, B. Chimaraoke O. Izugbara. 2016 at <http://aphrc.org/wp-content/uploads/2016/05/Maternal-Health-in-Nigeria_F...>
-
- NPC/Nigeria, N. P. C.- & International, I . Nigeria Demographic and Health Survey 2013. 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
