

In Vivo Validation of Elekta's Clarity Autoscan for Ultrasound-based Intrafraction Motion Estimation of the Prostate During Radiation Therapy
- PMID: 29859785
- PMCID: PMC6202949
- DOI: 10.1016/j.ijrobp.2018.04.008
In Vivo Validation of Elekta's Clarity Autoscan for Ultrasound-based Intrafraction Motion Estimation of the Prostate During Radiation Therapy
Abstract
Purpose: Our purpose was to perform an in vivo validation of ultrasound imaging for intrafraction motion estimation using the Elekta Clarity Autoscan system during prostate radiation therapy. The study was conducted as part of the Clarity-Pro trial (NCT02388308).
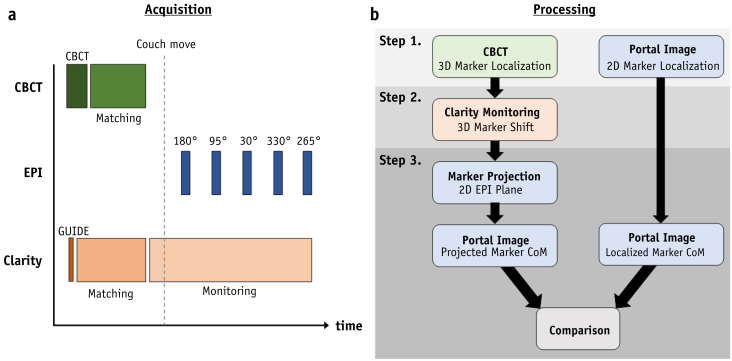
Methods and materials: Initial locations of intraprostatic fiducial markers were identified from cone beam computed tomography scans. Marker positions were translated according to Clarity intrafraction 3-dimensional prostate motion estimates. The updated locations were projected onto the 2-dimensional electronic portal imager plane. These Clarity-based estimates were compared with the actual portal-imaged 2-dimensional marker positions. Images from 16 patients encompassing 80 fractions were analyzed. To investigate the influence of intraprostatic markers and image quality on ultrasound motion estimation, 3 observers rated image quality, and the marker visibility on ultrasound images was assessed.
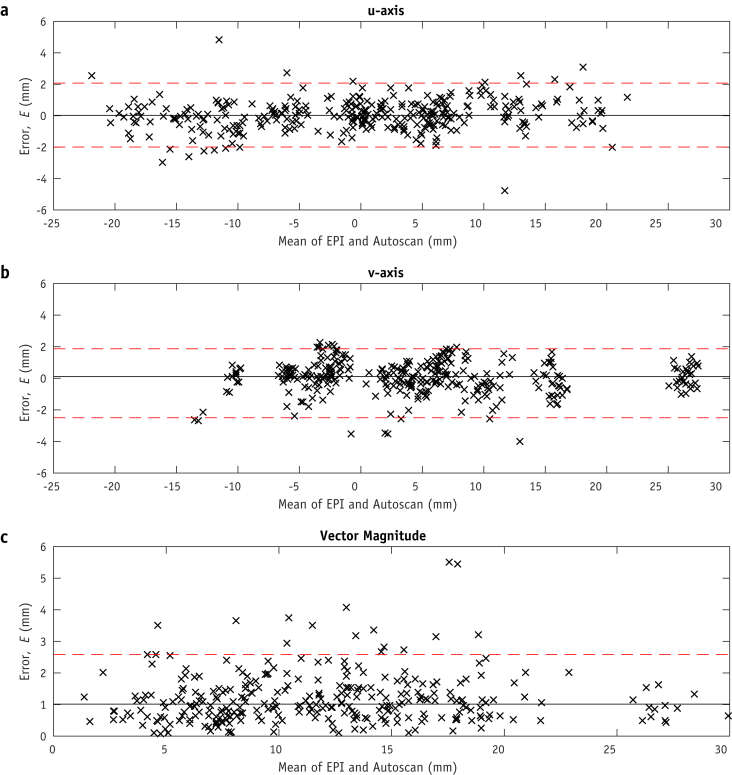
Results: The median difference between Clarity-defined intrafraction marker locations and portal-imaged marker locations was 0.6 mm (with 95% limit of agreement at 2.5 mm). Markers were identified on ultrasound in only 3 of a possible 240 instances. No linear relationship between image quality and Clarity motion estimation confidence was identified. The difference between Clarity-based motion estimates and electronic portal-imaged marker location was also independent of image quality. Clarity estimation confidence was degraded in a single fraction owing to poor probe placement.
Conclusions: The accuracy of Clarity intrafraction prostate motion estimation is comparable with that of other motion-monitoring systems in radiation therapy. The effect of fiducial markers in the study was deemed negligible as they were rarely visible on ultrasound images compared with intrinsic anatomic features. Clarity motion estimation confidence was robust to variations in image quality and the number of ultrasound-imaged anatomic features; however, it was degraded as a result of poor probe placement.
Copyright © 2018 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Miralbell R., Roberts S.A., Zubizarreta E. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: Alpha/beta = 1.4 (0.9-2.2) Gy. Int J Radiat Oncol Biol Phys. 2012;82:e17–e24. - PubMed
-
- Clemente S., Nigro R., Oliviero C. Role of the technical aspects of hypofractionated radiation therapy treatment of prostate cancer: A review. Int J Radiat Oncol Biol Phys. 2015;91:182–195. - PubMed
-
- Tree A.C., Khoo V.S., Van As N.J. Is biochemical relapse-free survival after profoundly hypofractionated radiotherapy consistent with current radiobiological models? Clin Oncol. 2014;26:216–229. - PubMed
-
- King C.R., Freeman D., Kaplan I. Stereotactic body radiotherapy for localized prostate cancer: Pooled analysis from a multi-institutional consortium of prospective phase II trials. Radiother Oncol. 2013;109:217–221. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
