

Are We on Our Way to Achieving the 2020 Goals for Schistosomiasis Morbidity Control Using Current World Health Organization Guidelines?
- PMID: 29860290
- PMCID: PMC5982704
- DOI: 10.1093/cid/ciy001
Are We on Our Way to Achieving the 2020 Goals for Schistosomiasis Morbidity Control Using Current World Health Organization Guidelines?
Abstract
Background: Schistosomiasis remains an endemic parasitic disease affecting millions of people around the world. The World Health Organization (WHO) has set goals of controlling morbidity to be reached by 2020, along with elimination as a public health problem in certain regions by 2025. Mathematical models of parasite transmission and treatment impact have been developed to assist in controlling the morbidity caused by schistosomiasis. These models can inform and guide implementation policy for mass drug administration programs, and help design monitoring and evaluation activities.
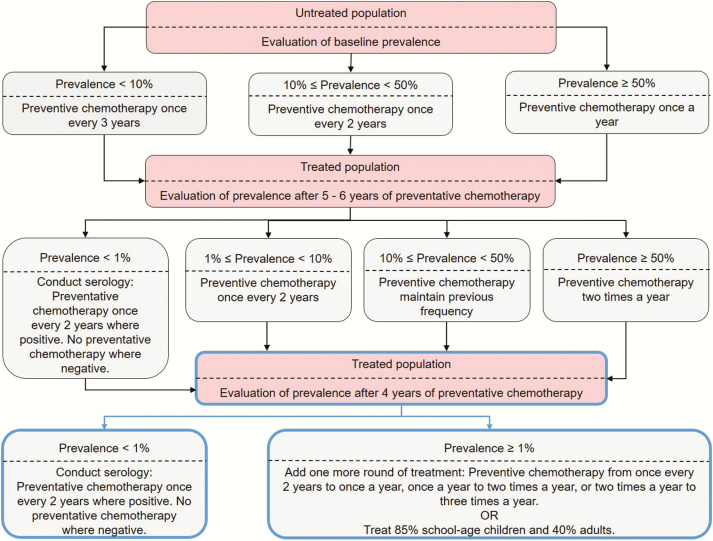
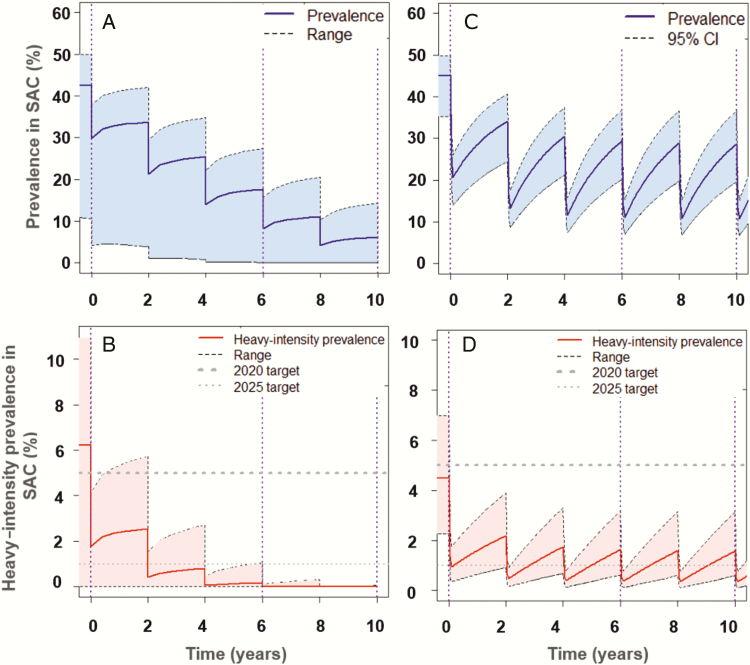
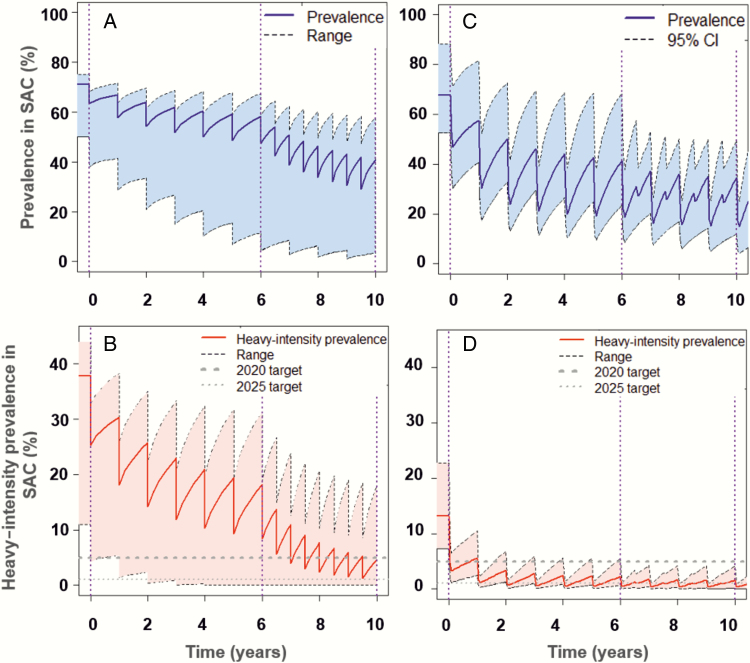
Methods: We use these models to predict whether the guidelines set by the WHO are on track for achieving their 2020 goal for the control of morbidity, specifically for Schistosoma mansoni. We examine whether programmatic adaptations; namely increases in treatment coverage and/or expansion to adult inclusion in treatment, will improve the likelihood of reaching the WHO goals.
Results: We find that in low-prevalence settings, the goals are likely to be attainable under current WHO guidelines, but in moderate to high-prevalence settings, the goals are less likely to be achieved unless treatment coverage is increased and expanded to at least 85% for school-aged children and 40% for adults.
Conclusions: To improve the likelihood of reaching the WHO goals, programmatic adaptations are required, particularly for moderate- to high-prevalence settings. Furthermore, improvements in adherence to treatment, potential development of candidate vaccines, and enhanced snail control and WASH (water, sanitation, and hygiene) measures will all assist in achieving the goals.
Figures
References
-
- London Declaration on Neglected Tropical Diseases. Available at: http://unitingtocombatntds.org/. Accessed 24 April 2017.
-
- World Health Organization. Schistosomiasis: progress report 2001–2011 and strategic plan 2012–2020. Geneva, Switzerland: WHO, 2013.
-
- Anderson RM, Turner HC, Farrell SH, Truscott JE. Studies of the transmission dynamics, mathematical model development and the control of schistosome parasites by mass drug administration in human communities. Adv Parasitol 2016; 94:199–246. - PubMed
-
- Sturrock RF. The schistosomes and their intermediate hosts. In: Mahmoud AAF. ed. Schistosomiasis. London: Imperial College Press, 2001:7–83.
-
- King CH, Dickman K, Tisch DJ. Reassessment of the cost of chronic helmintic infection: a meta-analysis of disability-related outcomes in endemic schistosomiasis. Lancet 2005; 365:1561–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
