

Defining Survivorship Trajectories Across Patients With Solid Tumors: An Evidence-Based Approach
- PMID: 29860375
- PMCID: PMC6248088
- DOI: 10.1001/jamaoncol.2018.2761
Defining Survivorship Trajectories Across Patients With Solid Tumors: An Evidence-Based Approach
Abstract
Importance: Survivorship involves a multidisciplinary approach to surveillance and management of comorbidities and secondary cancers, overseen by oncologists, surgeons, and primary care physicians. Optimal timing and coordination of care, however, is unclear and often based on arbitrary 5-year cutoffs.
Objective: To determine high- and low-risk periods for all tumor types that could define when survivorship care might best be overseen by oncologists and when to transition to primary care physicians.
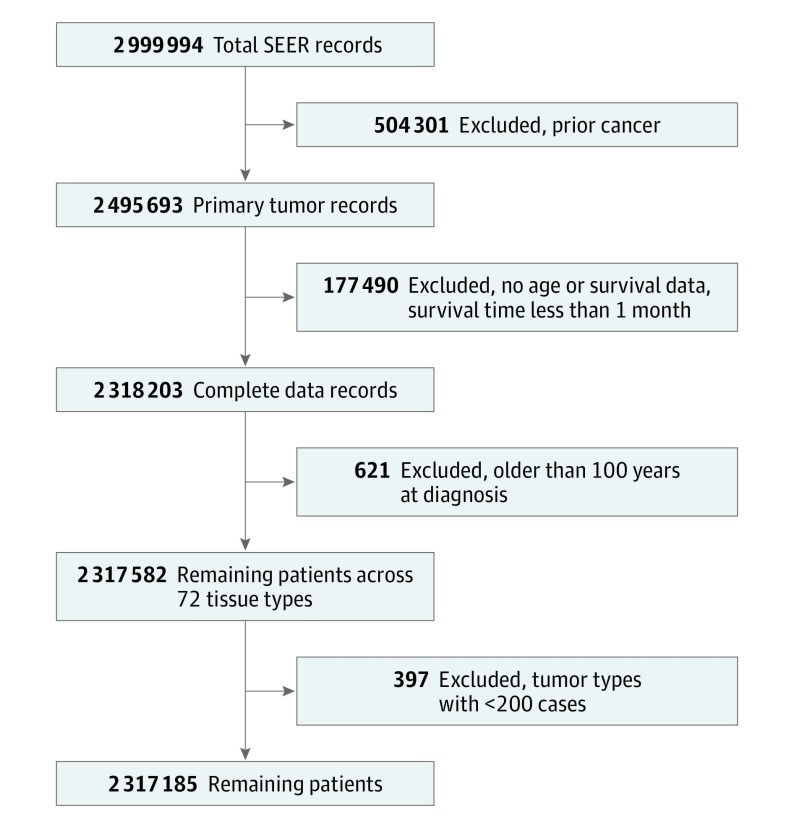
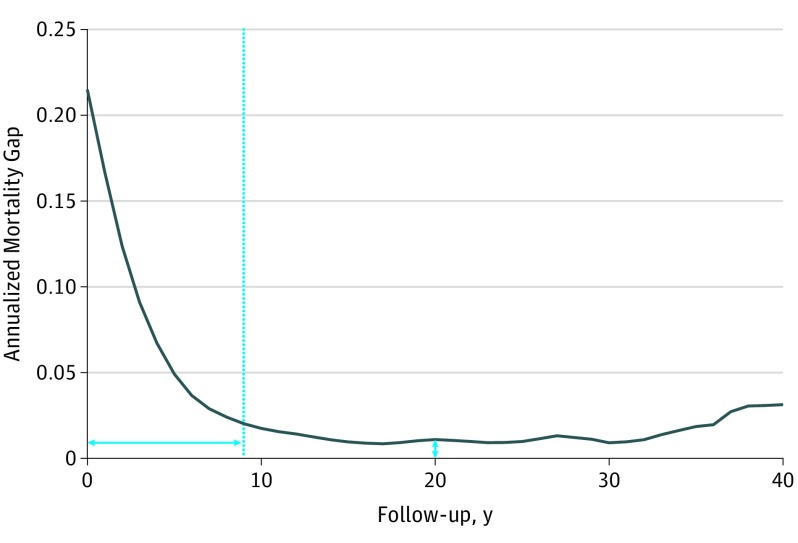
Design, setting, and participants: In this pan-cancer, longitudinal, observational study, excess mortality hazard, calculated as an annualized mortality risk above a baseline population, was plotted over time. The time this hazard took to stabilize defined a high-risk period. The percent morality elevation above age- and sex-matched controls in the latter low-risk period was reported as a mortality gap. The US population-based Surveillance, Epidemiology, and End Results database defined the cancer population, and the US Census life tables defined controls. Incident cases of patients with cancer were separated into tumor types based on International Classification of Diseases for Oncology definitions.
Exposures: Population-level data on incident cancer cases was compared with the general US population.
Main outcomes and measures: Overall mortality and cause of death were reported on observed cancer cases.
Results: A total of 2 317 185 patients (median age, 63 years; 49.8% female) with 66 primary tumor types were evaluated. High-risk surveillance period durations ranged from less than 1 year (breast, prostate, lip, ocular, and parathyroid cancers) up to 19 years (unspecified gastrointestinal cancers). The annualized mortality gap, representing the excess mortality in the stable period, ranged from a median 0.26% to 9.33% excess annual mortality (thyroid and hypopharyngeal cancer populations, respectively). Cluster analysis produced 6 risk cluster groups: group 1, with median survival of 16.2 (5th to 95th percentile range [PR], 10.7-40.2) years and median high-risk period of 2.5 (PR, 0-5.0) years; group 2, 8.3 (PR, 5.1-23.3) and 2.5 (PR, 4.0-8.0) years; group 3, 2.8 (PR, 1.4-3.7) and 7.0 (PR, 6.0-11.1) years; group 4, 1.6 (PR, 1.5-1.8) and 6.0 (PR, 5.1-11.4) years; group 5, 0.8 (PR, 0.5-1.2) and 0.8 (PR, 0.5-1.2) years; and group 6, 0.5 (PR, 0.4-0.8) and 12.0 (PR, 9.3-12.9) years, respectively. Subanalyses of selected tumor types in these groups revealed that stratifying on stage and histologic type can change the risk cluster and guidance for care.
Conclusions and relevance: These findings indicate that a standardized 5-year surveillance period is inadequate for some cancers while excessive for others. High-risk cancers require the most resources with the longest high-risk period, highest persistent baseline mortality risk, and longest period of primary cancer mortality, all arguing for longer follow-up with an oncologist in these cancers.
Conflict of interest statement
Figures
Comment in
-
Better Guidelines Needed for Cancer Survivorship Management.CA Cancer J Clin. 2018 Nov;68(6):392-393. doi: 10.3322/caac.21435. Epub 2018 Oct 9. CA Cancer J Clin. 2018. PMID: 30300452 No abstract available.
References
-
- Hewitt M, Greenfield S, Stovall E, eds. From Cancer Patient to Cancer Survivor. Washington, DC: National Academies Press; 2005. doi:10.17226/11468 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
