

Restenosis and risk of stroke after stenting or endarterectomy for symptomatic carotid stenosis in the International Carotid Stenting Study (ICSS): secondary analysis of a randomised trial
- PMID: 29861139
- PMCID: PMC6004555
- DOI: 10.1016/S1474-4422(18)30195-9
Restenosis and risk of stroke after stenting or endarterectomy for symptomatic carotid stenosis in the International Carotid Stenting Study (ICSS): secondary analysis of a randomised trial
Abstract
Background: The risk of stroke associated with carotid artery restenosis after stenting or endarterectomy is unclear. We aimed to compare the long-term risk of restenosis after these treatments and to investigate if restenosis causes stroke in a secondary analysis of the International Carotid Stenting Study (ICSS).
Methods: ICSS is a parallel-group randomised trial at 50 tertiary care centres in Europe, Australia, New Zealand, and Canada. Patients aged 40 years or older with symptomatic carotid stenosis measuring 50% or more were randomly assigned either stenting or endarterectomy in a 1:1 ratio. Randomisation was computer-generated and done centrally, with allocation by telephone or fax, stratified by centre, and with minimisation for sex, age, side of stenosis, and occlusion of the contralateral carotid artery. Patients were followed up both clinically and with carotid duplex ultrasound at baseline, 30 days after treatment, 6 months after randomisation, then annually for up to 10 years. We included patients whose assigned treatment was completed and who had at least one ultrasound examination after treatment. Restenosis was defined as any narrowing of the treated artery measuring 50% or more (at least moderate) or 70% or more (severe), or occlusion of the artery. The degree of restenosis based on ultrasound velocities and clinical outcome events were adjudicated centrally; assessors were masked to treatment assignment. Restenosis was analysed using interval-censored models and its association with later ipsilateral stroke using Cox regression. This trial is registered with the ISRCTN registry, number ISRCTN25337470. This report presents a secondary analysis, and follow-up is complete.
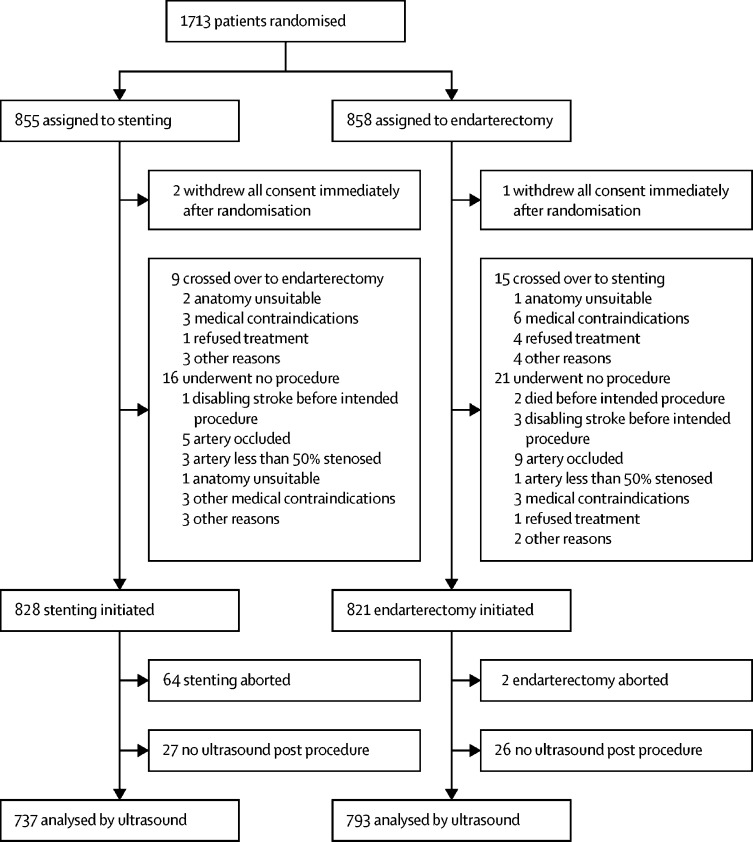
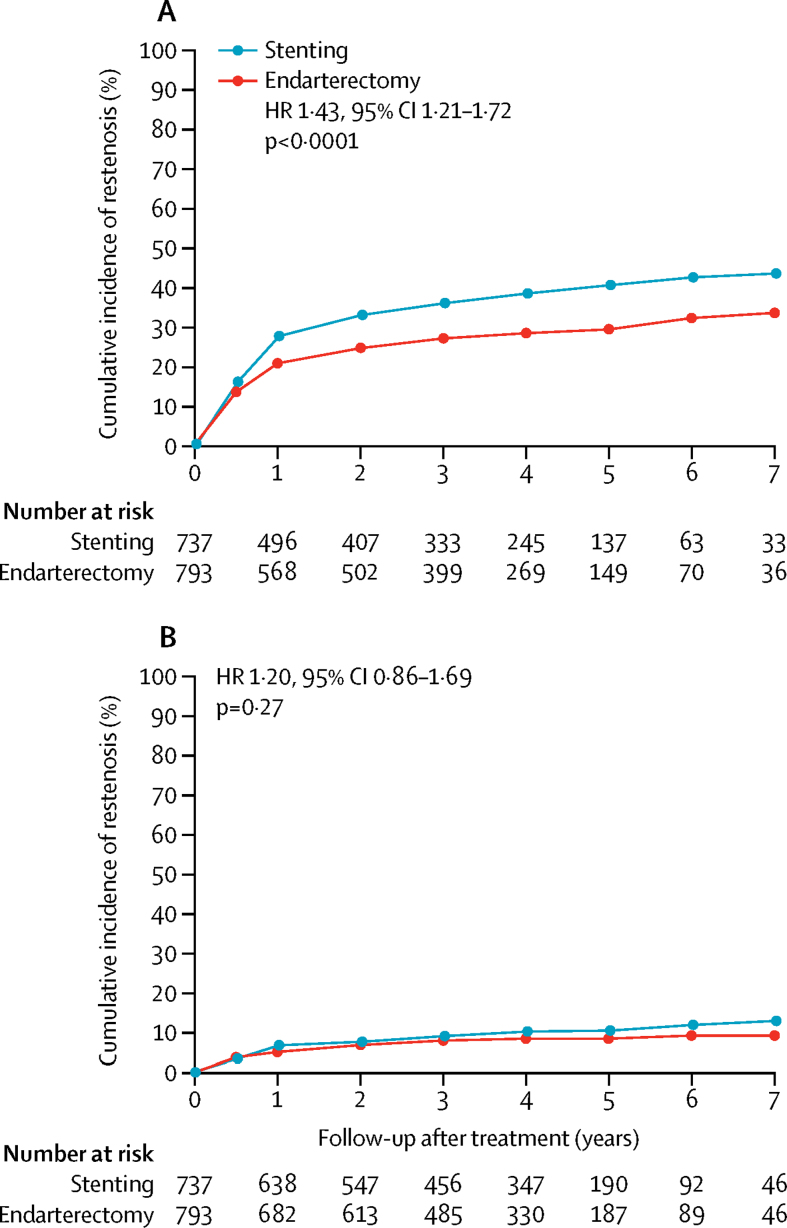
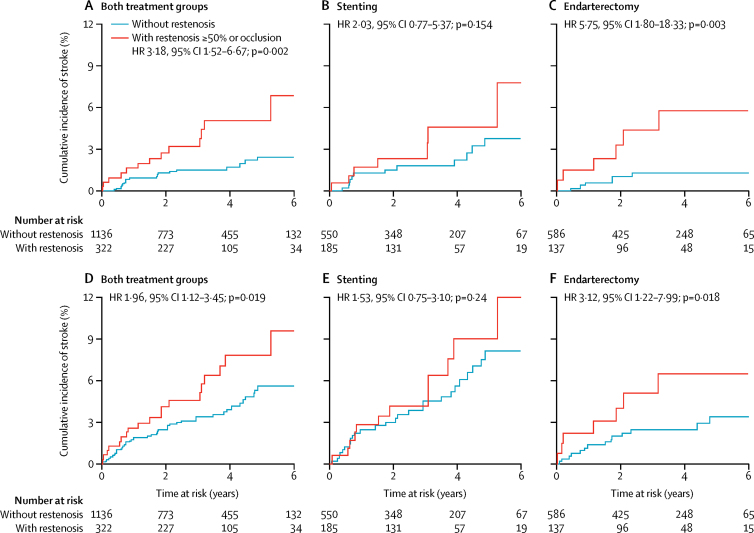
Findings: Between May, 2001, and October, 2008, 1713 patients were enrolled and randomly allocated treatment (855 were assigned stenting and 858 endarterectomy), of whom 1530 individuals were followed up with ultrasound (737 assigned stenting and 793 endarterectomy) for a median of 4·0 years (IQR 2·3-5·0). At least moderate restenosis (≥50%) occurred in 274 patients after stenting (cumulative 5-year risk 40·7%) and in 217 after endarterectomy (29·6%; unadjusted hazard ratio [HR] 1·43, 95% CI 1·21-1·72; p<0·0001). Patients with at least moderate restenosis (≥50%) had a higher risk of ipsilateral stroke than did individuals without restenosis in the overall patient population (HR 3·18, 95% CI 1·52-6·67; p=0·002) and in the endarterectomy group alone (5·75, 1·80-18·33; p=0·003), but no significant increase in stroke risk after restenosis was recorded in the stenting group (2·03, 0·77-5·37; p=0·154; p=0·10 for interaction with treatment). No difference was noted in the risk of severe restenosis (≥70%) or subsequent stroke between the two treatment groups.
Interpretation: At least moderate (≥50%) restenosis occurred more frequently after stenting than after endarterectomy and increased the risk for ipsilateral stroke in the overall population. Whether the restenosis-mediated risk of stroke differs between stenting and endarterectomy requires further research.
Funding: Medical Research Council, the Stroke Association, Sanofi-Synthélabo, and the European Union.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access Article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Is surveillance for restenosis justified after carotid revascularisation?Lancet Neurol. 2018 Jul;17(7):570-571. doi: 10.1016/S1474-4422(18)30199-6. Epub 2018 Jun 1. Lancet Neurol. 2018. PMID: 29861140 No abstract available.
-
The fate of severe restenosis after carotid interventions.Lancet Neurol. 2018 Oct;17(10):842-843. doi: 10.1016/S1474-4422(18)30315-6. Epub 2018 Sep 18. Lancet Neurol. 2018. PMID: 30264723 No abstract available.
-
The fate of severe restenosis after carotid interventions - Authors' reply.Lancet Neurol. 2018 Oct;17(10):843-844. doi: 10.1016/S1474-4422(18)30321-1. Epub 2018 Sep 18. Lancet Neurol. 2018. PMID: 30264724 No abstract available.
References
-
- Mas JL, Chatellier G, Beyssen B. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660–1671. - PubMed
-
- The SPACE Collaborative Group 30 day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet. 2006;368:1239–1247. - PubMed
-
- Eckstein H-H, Ringleb P, Allenberg J-R. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol. 2008;7:893–902. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
