

The challenges of diagnosing osteoporosis and the limitations of currently available tools
- PMID: 29862042
- PMCID: PMC5975657
- DOI: 10.1186/s40842-018-0062-7
The challenges of diagnosing osteoporosis and the limitations of currently available tools
Abstract
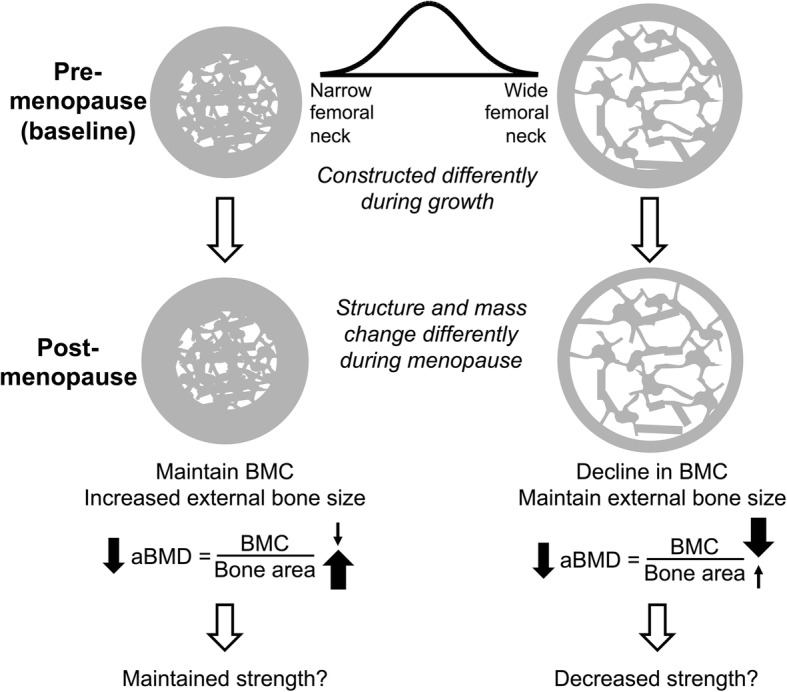
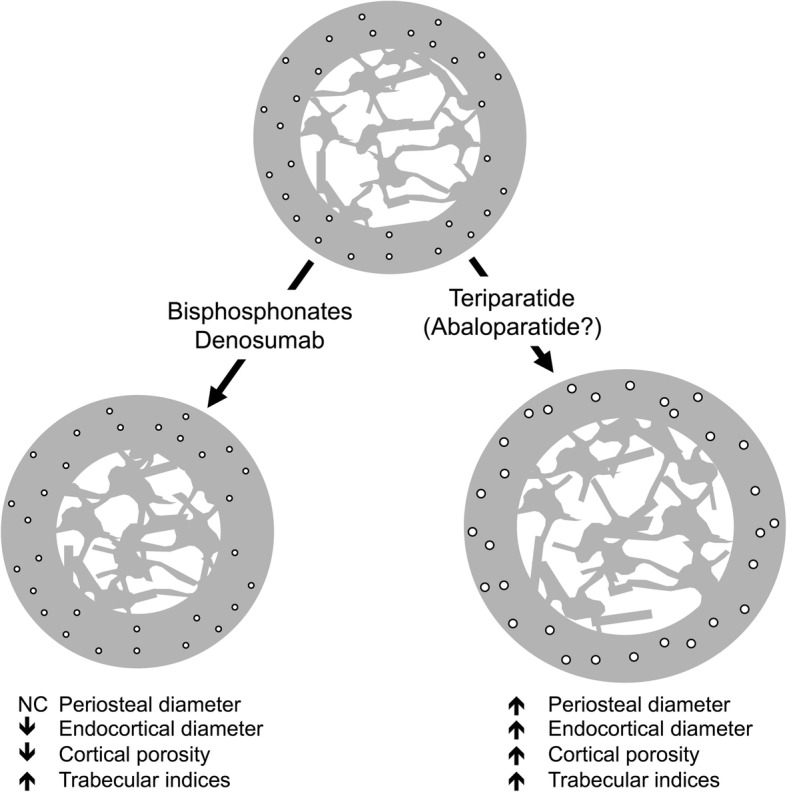
Dual-energy X-ray absorptiometry (DXA) was the first imaging tool widely utilized by clinicians to assess fracture risk, especially in postmenopausal women. The development of DXA nearly coincided with the availability of effective osteoporosis medications. Although osteoporosis in adults is diagnosed based on a T-score equal to or below - 2.5 SD, most individuals who sustain fragility fractures are above this arbitrary cutoff. This incongruity poses a challenge to clinicians to identify patients who may benefit from osteoporosis treatments. DXA scanners generate 2 dimensional images of complex 3 dimensional structures, and report bone density as the quotient of the bone mineral content divided by the bone area. An obvious pitfall of this method is that a larger bone will convey superior strength, but may in fact have the same bone density as a smaller bone. Other imaging modalities are available such as peripheral quantitative CT, but are largely research tools. Current osteoporosis medications increase bone density and reduce fracture risk but the mechanisms of these actions vary. Anti-resorptive medications (bisphosphonates and denosumab) primarily increase endocortical bone by bolstering mineralization of endosteal resorption pits and thereby increase cortical thickness and reduce cortical porosity. Anabolic medications (teriparatide and abaloparatide) increase the periosteal and endosteal perimeters without large changes in cortical thickness resulting in a larger more structurally sound bone. Because of the differences in the mechanisms of the various drugs, there are likely benefits of selecting a treatment based on a patient's unique bone structure and pattern of bone loss. This review retreats to basic principles in order to advance clinical management of fragility fractures by examining how skeletal biomechanics, size, shape, and ultra-structural properties are the ultimate predictors of bone strength. Accurate measurement of these skeletal parameters through the development of better imaging scanners is critical to advancing fracture risk assessment and informing clinicians on the best treatment strategy. With this information, a "treat to target" approach could be employed to tailor current and future therapies to each patient's unique skeletal characteristics.
Keywords: Bisphosphonates; Denosumab; Dual X-ray absorptiometry; Osteoporosis; Peripheral quantitative computed tomography; Romosozumab; Skeletal biomechanics; Skeletal fracture; Teriparatide.
Conflict of interest statement
Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- What is Osteoporosis and What Causes It? Arlington: National Osteoporosis Foundation. https://www.nof.org/patients/what-is-osteoporosis/.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
