

Everolimus Plus Exemestane vs Everolimus or Capecitabine Monotherapy for Estrogen Receptor-Positive, HER2-Negative Advanced Breast Cancer: The BOLERO-6 Randomized Clinical Trial
- PMID: 29862411
- PMCID: PMC6233772
- DOI: 10.1001/jamaoncol.2018.2262
Everolimus Plus Exemestane vs Everolimus or Capecitabine Monotherapy for Estrogen Receptor-Positive, HER2-Negative Advanced Breast Cancer: The BOLERO-6 Randomized Clinical Trial
Abstract
Importance: Everolimus plus exemestane and capecitabine are approved second-line therapies for advanced breast cancer.
Objective: A postapproval commitment to health authorities to estimate the clinical benefit of everolimus plus exemestane vs everolimus or capecitabine monotherapy for estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer.
Design: Open-label, randomized, phase 2 trial of treatment effects in postmenopausal women with advanced breast cancer that had progressed during treatment with nonsteroidal aromatase inhibitors.
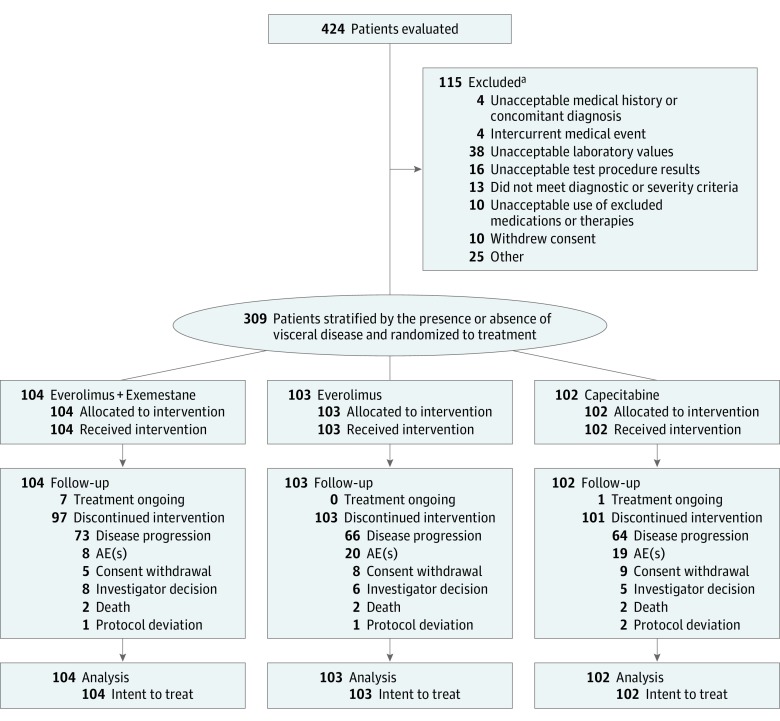
Interventions: Patients were randomized to 3 treatment regimens: (1) everolimus (10 mg/d) plus exemestane (25 mg/d); (2) everolimus alone (10 mg/d); and (3) capecitabine alone (1250 mg/m2 twice daily).
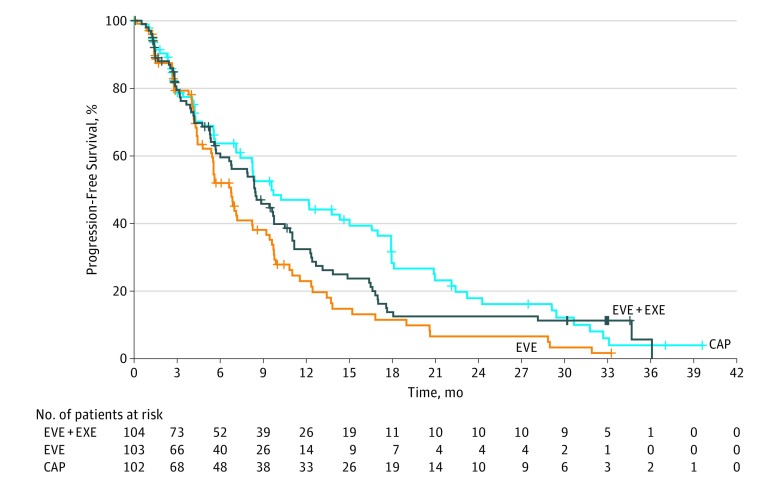
Main outcomes and measures: Estimated hazard ratios (HRs) of progression-free survival (PFS) for everolimus plus exemestane vs everolimus alone (primary objective) or capecitabine alone (key secondary objective). Safety was a secondary objective. No formal statistical comparisons were planned.
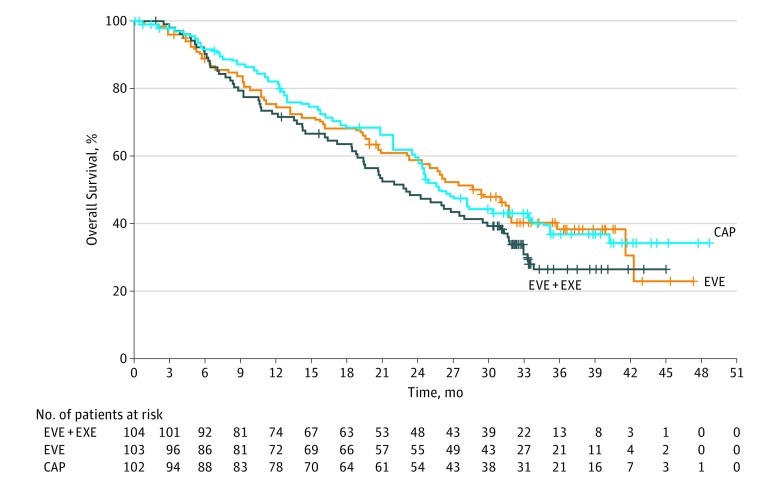
Results: A total of 309 postmenopausal women were enrolled, median age, 61 years (range, 32-88 years). Of these, 104 received everolimus plus exemestane; 103, everolimus alone; and 102, capecitabine alone. Median follow-up from randomization to the analysis cutoff (June 1, 2017) was 37.6 months. Estimated HR of PFS was 0.74 (90% CI, 0.57-0.97) for the primary objective of everolimus plus exemestane vs everolimus alone and 1.26 (90% CI, 0.96-1.66) for everolimus plus exemestane vs capecitabine alone. Between treatment arms, potential informative censoring was noted, and a stratified multivariate Cox regression model was used to account for imbalances in baseline characteristics; a consistent HR was observed for everolimus plus exemestane vs everolimus (0.73; 90% CI, 0.56-0.97), but the HR was closer to 1 for everolimus plus exemestane vs capecitabine (1.15; 90% CI, 0.86-1.52). Grade 3 to 4 adverse events were more frequent with capecitabine (74%; n = 75) vs everolimus plus exemestane (70%; n = 73) or everolimus alone (59%; n = 61). Serious adverse events were more frequent with everolimus plus exemestane (36%; n = 37) vs everolimus alone (29%; n = 30) or capecitabine (29%; n = 30).
Conclusions and relevance: These findings suggest that everolimus plus exemestane combination therapy offers a PFS benefit vs everolimus alone, and they support continued use of this therapy in this setting. A numerical PFS difference with capecitabine vs everolimus plus exemestane should be interpreted cautiously owing to imbalances among baseline characteristics and potential informative censoring.
Trial registration: ClinicalTrials.gov identifier: NCT01783444.
Conflict of interest statement
Figures
References
-
- National Comprehensive Cancer Network (NCCN) NCCN clinical practice guidelines in oncology (NCCN guidelines): breast cancer; V1. 2018. https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed May 11, 2018.
-
- Robert NJ, Diéras V, Glaspy J, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J Clin Oncol. 2011;29(10):1252-1260. doi: 10.1200/JCO.2010.28.0982 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
