

Increased risk of aminoglycoside-induced hearing loss in MDR-TB patients with HIV coinfection
- PMID: 29862952
- PMCID: PMC6002855
- DOI: 10.5588/ijtld.17.0830
Increased risk of aminoglycoside-induced hearing loss in MDR-TB patients with HIV coinfection
Abstract
Setting: A high proportion of individuals with multidrug-resistant tuberculosis (MDR-TB) develop permanent hearing loss due to ototoxicity caused by injectable aminoglycosides (AGs). The prevalence of AG-induced hearing loss is greatest in tuberculosis (TB) and human immunodeficiency virus (HIV) endemic countries in sub-Saharan Africa. However, whether HIV coinfection is associated with a higher incidence of AG-induced hearing loss during MDR-TB treatment is controversial.
Objective: To evaluate the impact of HIV coinfection on AG-induced hearing loss among individuals with MDR-TB in sub-Saharan Africa.
Design: This was a meta-analysis of articles published in PubMed, Embase, Scopus, Cumulative Index to Nursing and Allied Health Literature, Web of Science, Cochrane Review, and reference lists using search terms 'hearing loss', 'aminoglycoside', and 'sub-Saharan Africa'.
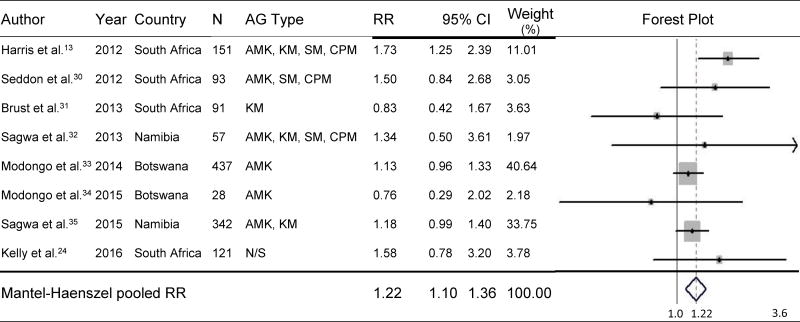
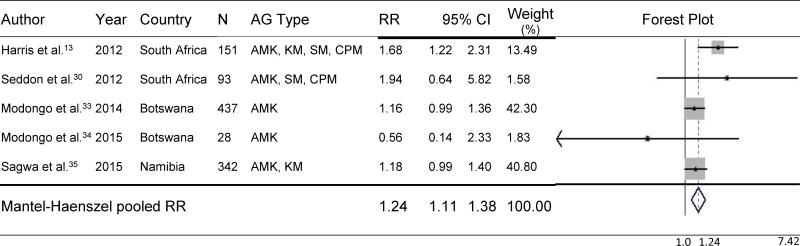
Results: Eight studies conducted in South Africa, Botswana and Namibia and published between 2012 and 2016 were included. As the included studies were homogeneous (χ2 = 8.84, df = 7), a fixed-effects model was used. Individuals with MDR-TB and HIV coinfection had a 22% higher risk of developing AG-induced hearing loss than non-HIV-infected individuals (pooled relative risk 1.22, 95%CI 1.10-1.36) during MDR-TB treatment.
Conclusion: This finding is critical for TB programs with regard to the expansion of injectable-sparing regimens. Our findings lend credibility to using injectable-sparing regimens and more frequent hearing monitoring, particularly in resource-limited settings for HIV-coinfected individuals.
Figures
Comment in
-
Insufficient pharmacological research on TB drugs: new insights on safety are needed.Int J Tuberc Lung Dis. 2018 Jun 1;22(6):593. doi: 10.5588/ijtld.18.0287. Int J Tuberc Lung Dis. 2018. PMID: 29862940 No abstract available.
References
-
- Republic of South Africa Department of Health. Management of drug-resistant tuberculosis: policy guidelines. Vol. 161. Pretoria, Republic of South Africa: Department of Health; 2013.
-
- World Health Organization. WHO treatment guidelines for drug-resistant tuberculosis, 2016 updates. Geneva, Switzerland: WHO; 2016.
-
- Caminero JA, Sotgiu G, Zumla A, Migliori GB. Best drug treatment for multidrug-resistant and extensively drug-resistant tuberculosis. Lancet Infect Dis. 2010;10:621–629. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
