

Early Infections Complicating the Care of Combat Casualties from Iraq and Afghanistan
- PMID: 29863446
- PMCID: PMC5867509
- DOI: 10.1089/sur.2017.240
Early Infections Complicating the Care of Combat Casualties from Iraq and Afghanistan
Abstract
Background: During the conflicts in Iraq and Afghanistan, more than 52,000 U.S. military members were wounded in action. The battlefield mortality rate was lower than in past conflicts, however, those surviving often had complex soft tissue and bone injuries requiring multiple surgeries. This report describes the rates, types, and risks of infections complicating the care of combat casualties.
Patients and methods: Infection and microbiology data obtained from the Trauma Infectious Disease Outcomes Study (TIDOS), a prospective observational study of infections complicating deployment-related injuries, were used to determine the proportion of infection, types, and associated organisms. Injury and surgical information were collected from the Department of Defense Trauma Registry. Multivariable Cox proportional hazards and logistic regression models were used to evaluate potential factors associated with infection.
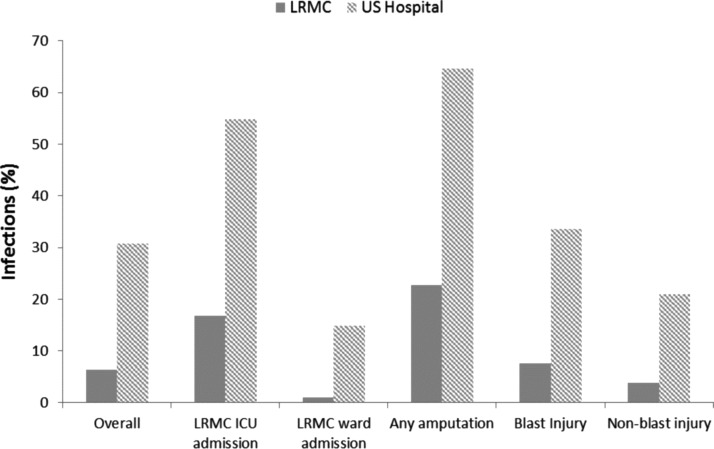
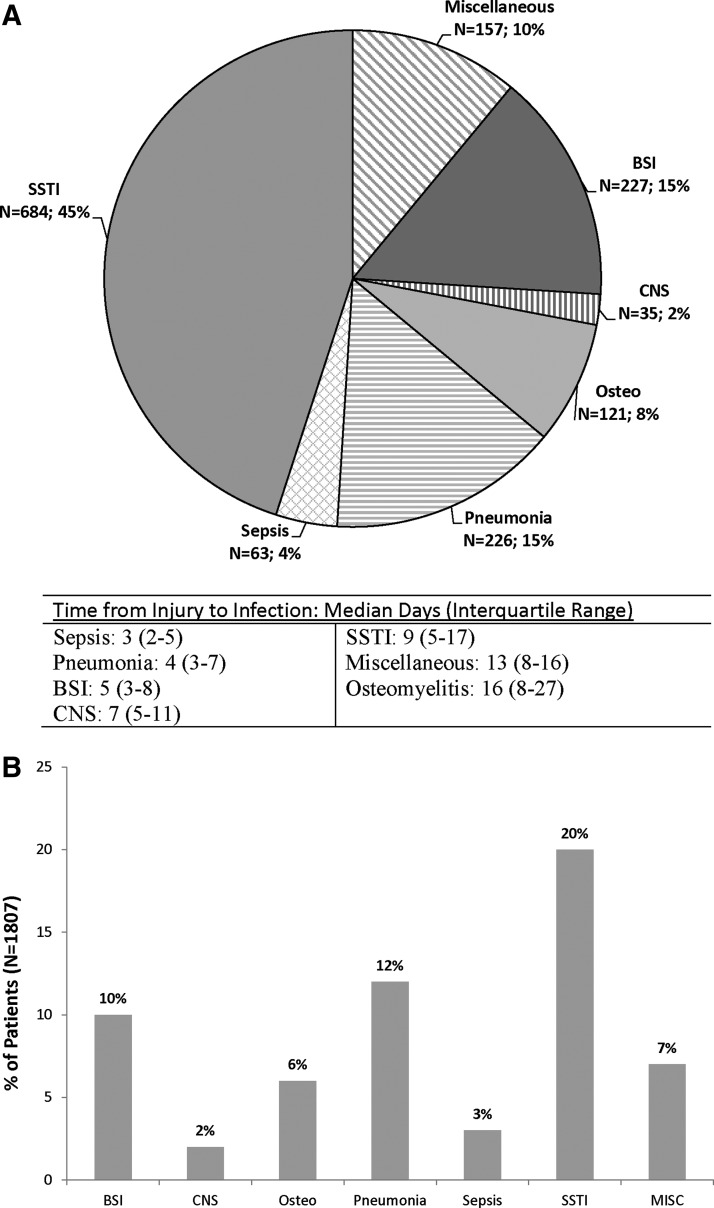
Results: From 2009-2012, 1,807 combat casualties were evacuated to U.S. TIDOS-participating hospitals. Among the 1,807 patients, the proportion of overall infections from time of injury through initial U.S. hospitalization was 34% with half being skin, soft tissue, or bone infections. Infected wounds most commonly grew Enterococcus faecium, Pseudomonas aeruginosa, Acinetobacter spp. or Escherichia coli. In the multivariable model, amputation, blood transfusions, intensive care unit admission, injury severity scores, mechanical ventilation, and mechanism of injury were associated with risk of infection.
Conclusions: One-third of combat casualties from Iraq and Afghanistan develop infections during their initial hospitalization. Amputations, blood transfusions, and overall injury severity are associated with risk of infection, whereas more easily modifiable factors such as early operative intervention or antibiotic administration are not.
Keywords: combat trauma; military health; trauma-related infections; wound infections.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Murray CK, Hinkle MK, Yun HC. History of infections associated with combat-related injuries. J Trauma 2008;64:S221–S231 - PubMed
-
- Hardaway RM., 3rd. Viet Nam wound analysis. J Trauma 1978;18:635–643 - PubMed
-
- North JP. Clostridial wound infections and gas gangrene; Arterial damage as a modifying factor. Surgery 1947;21:364–372 - PubMed
-
- Neel HB, Cole JP. Gas gangrene in amphibious warfare in the Pacific area. Am J Surg 1944;66:290–299
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
