

Donor-specific Antibody Surveillance and Graft Outcomes in Pediatric Kidney Transplant Recipients
- PMID: 29863579
- PMCID: PMC6249093
- DOI: 10.1097/TP.0000000000002310
Donor-specific Antibody Surveillance and Graft Outcomes in Pediatric Kidney Transplant Recipients
Abstract
Background: The development of de novo donor-specific antibodies (dnDSA) has been associated with rejection and graft loss in kidney transplantation, and DSA screening is now recommended in all kidney transplant recipients. However, the clinical significance of dnDSA detected by screening patients with a stable creatinine remains unclear.
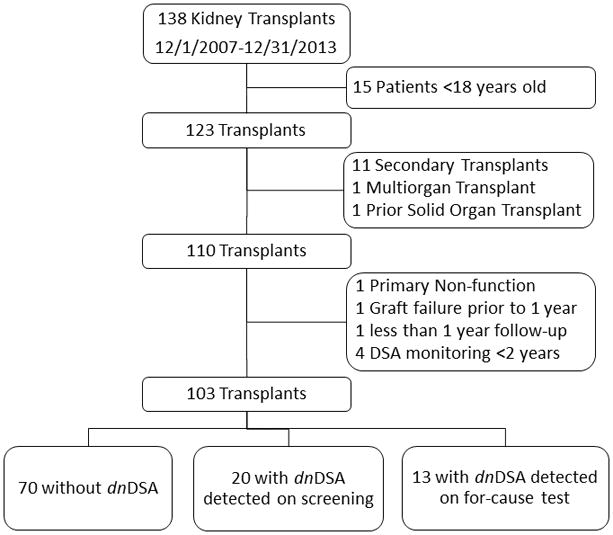
Methods: One hundred three patients younger than 18years receiving a first, kidney alone transplant between December 1, 2007, and December 31, 2013, underwent DSA screening every 3months for 2years posttransplant, with additional testing as clinically indicated. No treatment was given for DSAs in the absence of biopsy-proven rejection.
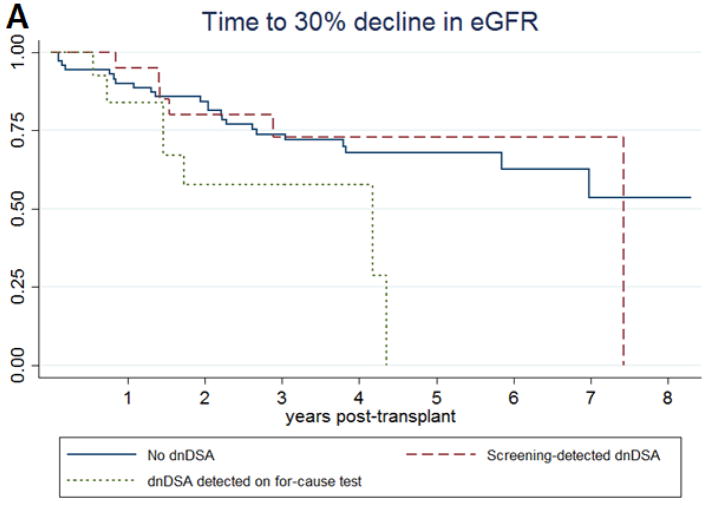
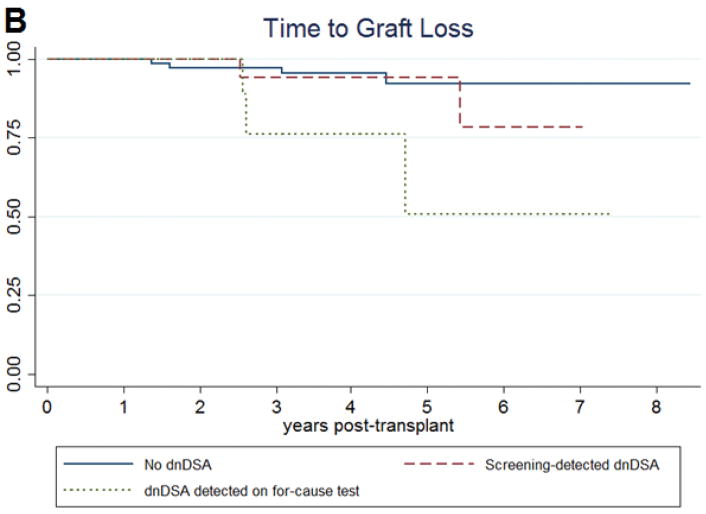
Results: Twenty (19%) patients had dnDSA first detected on a screening test, and 13 (13%) patients had dnDSA first detected on a for-cause test. Mean follow-up time posttransplant was 4.4years. Screening-detected dnDSA was associated with an increased risk of rejection within 3years, microvascular inflammation, and C4d staining on a 2-year protocol biopsy. In a Cox proportional hazards regression, screening-detected dnDSA was not associated with time to 30% decline in estimated glomerular filtration rate (adjusted hazard ratio, 0.88; 95% confidence interval [CI], 0.30-2.00; P=0.598) or graft loss. dnDSA first detected on for-cause testing was associated with a 2.8 times increased risk of decline in graft function (95% CI, 1.08-7.27; P=0.034) and a 7.34 times increased risk of graft loss (95% CI, 1.37-39.23 P=0.020) compared with those who did not develop dnDSA.
Conclusions: The clinical setting in which dnDSA is first detected impacts the association between dnDSA and graft function. Further research is needed to clarify the role of dnDSA screening in pediatric kidney transplantation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Kim JJ, Balasubramanian R, Michaelides G, et al. The clinical spectrum of de novo donor-specific antibodies in pediatric renal transplant recipients. Am J Transplant. 2014;14(10):2350–2358. - PubMed
-
- Meier-Kriesche H-U, Schold JD, Kaplan B. Long-term renal allograft survival: have we made significant progress or is it time to rethink our analytic and therapeutic strategies? Am J Transplant. 2004;4(8):1289–1295. - PubMed
-
- El-Zoghby ZM, Stegall MD, Lager DJ, et al. Identifying specific causes of kidney allograft loss. Am J Transplant. 2009;9(3):527–535. - PubMed
-
- Terasaki PI. A personal perspective: 100-year history of the humoral theory of transplantation. Transplantation. 2012;93(8):751–756. - PubMed
-
- Christiaans MH, Overhof-de Roos R, Nieman F, van Hooff JP, van den Berg-Loonen EM. Donor-specific antibodies after transplantation by flow cytometry: relative change in fluorescence ratio most sensitive risk factor for graft survival. Transplantation. 1998;65(3):427–433. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
