

Race/Ethnicity and Sex and Opioid Administration in the Emergency Room
- PMID: 29863607
- PMCID: PMC6611165
- DOI: 10.1213/ANE.0000000000003517
Race/Ethnicity and Sex and Opioid Administration in the Emergency Room
Abstract
Background: Although racial/ethnic and sex disparities have been examined in health care generally and pain management more specifically, the combined influence of these sociodemographic factors together has not been well documented. The aim of this study was to examine the association between administration of opioid analgesics in the emergency department (ED) and interaction of race/ethnicity and sex.
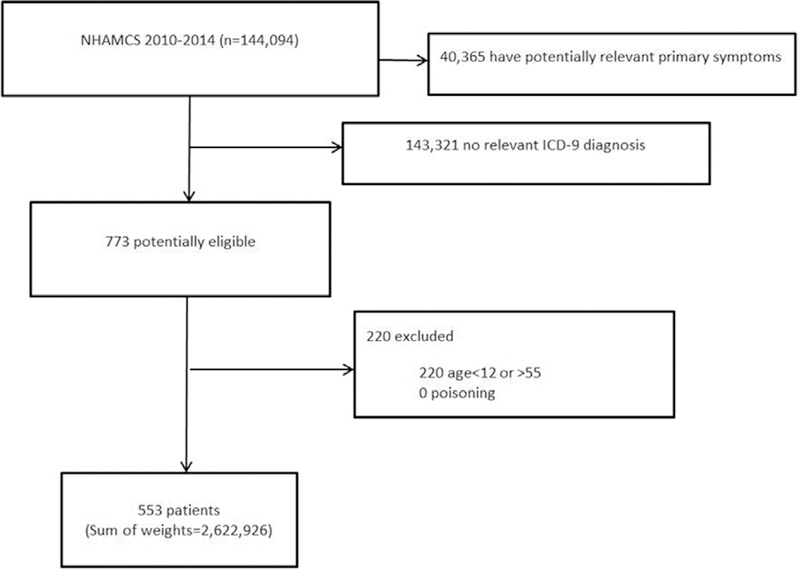
Methods: We conducted a retrospective cohort study using 2010-2014 Center for Disease Control-National Hospital Ambulatory Medical Care Survey data for patients 12-55 years of age presenting to EDs with a primary diagnosis of appendicitis or gallbladder disease as defined by International Classification of Diseases, Ninth Revision codes. The primary outcome was the receipt of opioid analgesic medications. Secondary outcomes included: receipt of nonopioids, receipt of antiemetic medications, wait time to see a provider, and length of visit in the ED. The association between sex and analgesic receipt within Caucasian non-Hispanic and non-Caucasian groups was evaluated adjusting for pain score on presentation, patient age, emergent status, number of comorbidities, time of visit (month, day of the week, standard versus nonstandard working hours, year), and US region.
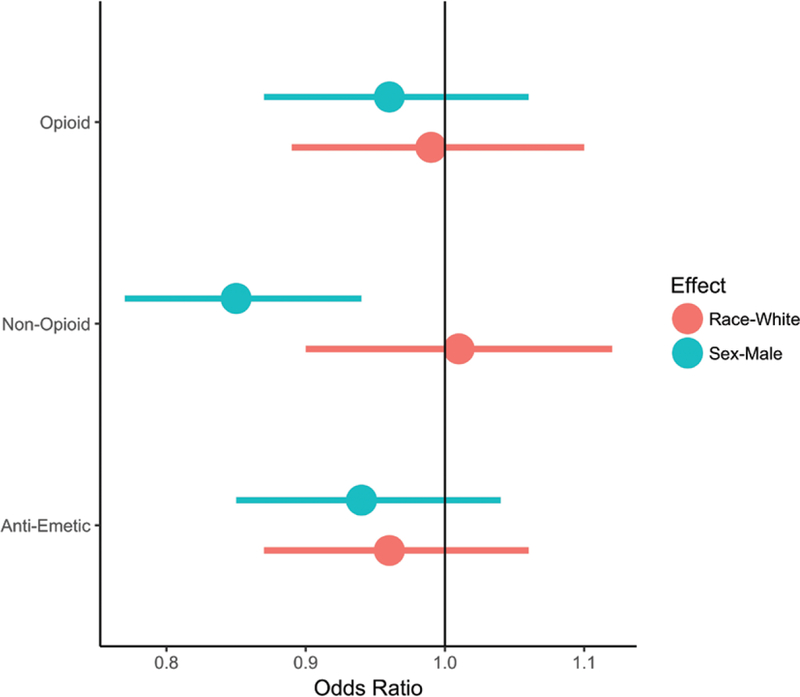
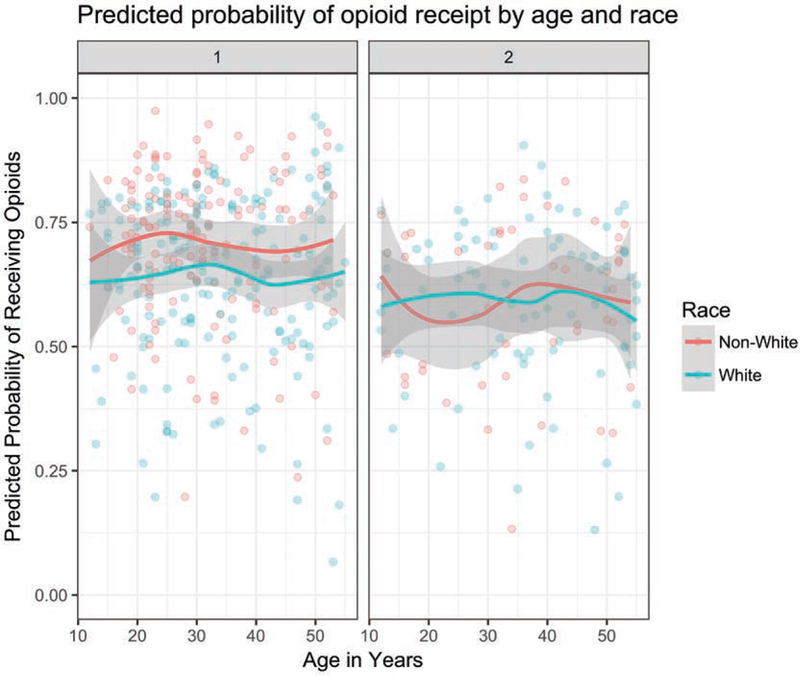
Results: After exclusions, a weighted sample of 553 ED visits was identified, representing 2,622,926 unique visits. The sample population was comprised of 1,858,035 (70.8%) females and 1,535,794 (58.6%) Caucasian non-Hispanics. No interaction was found in adjusted sampling-weighted model between sex and race/ethnicity on the odds of receiving opioids (P = .74). There was no difference in opioid administration to males as compared to females (odds ratio [OR] = 0.96, 95% CI, 0.87-1.06; P = .42) or to non-Caucasians as compared to Caucasians (OR = 0.99, 95% CI, 0.89-1.10; P = .84). In adjusted weighted models, non-Caucasian males, 123,121/239,457 (51.4%) did not differ from Caucasian non-Hispanic males, 317,427/525,434 (60.4%), on odds of receiving opioids, aOR = 0.88, 95% CI, 0.39-1.99; P = .75. Non-Caucasian females, 547,709/847,675 (64.6%) also did not differ from Caucasian females, 621,638/1,010,360 (61.5%), on odds of receiving opioids, aOR = 1.01, 95% CI, 0.53-1.90; P = .98. Across both sexes, non-Caucasians did not differ from Caucasians on receipt of nonopioid analgesics or antiemetics. Neither wait time to see a provider nor the length of the hospital visit was significantly different between sexes or race/ethnicities.
Conclusions: Based on National Hospital Ambulatory Medical Care Survey data from 2010 to 2014, there is no statistically significant interaction between race/ethnicity and sex for administration of opioid analgesia to people presenting to the ED with appendicitis or gallbladder disease. These results suggest that the joint effect of patient race/ethnicity and sex may not manifest in disparities in opioid management.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Comment on "Race/Ethnicity and Sex and Opioid Administration in the Emergency Room".Anesth Analg. 2019 May;128(5):e79. doi: 10.1213/ANE.0000000000003908. Anesth Analg. 2019. PMID: 30451724 No abstract available.
-
In Response.Anesth Analg. 2019 May;128(5):e79. doi: 10.1213/ANE.0000000000003909. Anesth Analg. 2019. PMID: 30451727 Free PMC article. No abstract available.
References
-
- Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington DC: NAP; 2003. - PubMed
-
- Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299:70–78. - PubMed
-
- Shah AA, Zogg CK, Zafar SN, et al. Analgesic access for acute abdominal pain in the emergency department among racial/ethnic minority patients: a nationwide examination. Med Care. 2015;53:1000–1009. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
