

Vitamin C: should we supplement?
- PMID: 29864039
- PMCID: PMC6039380
- DOI: 10.1097/MCC.0000000000000510
Vitamin C: should we supplement?
Abstract
Purpose of review: Hypovitaminosis C and vitamin C deficiency are very common in critically ill patients due to increased needs and decreased intake. Because vitamin C has pleiotropic functions, deficiency can aggravate the severity of illness and hamper recovery.
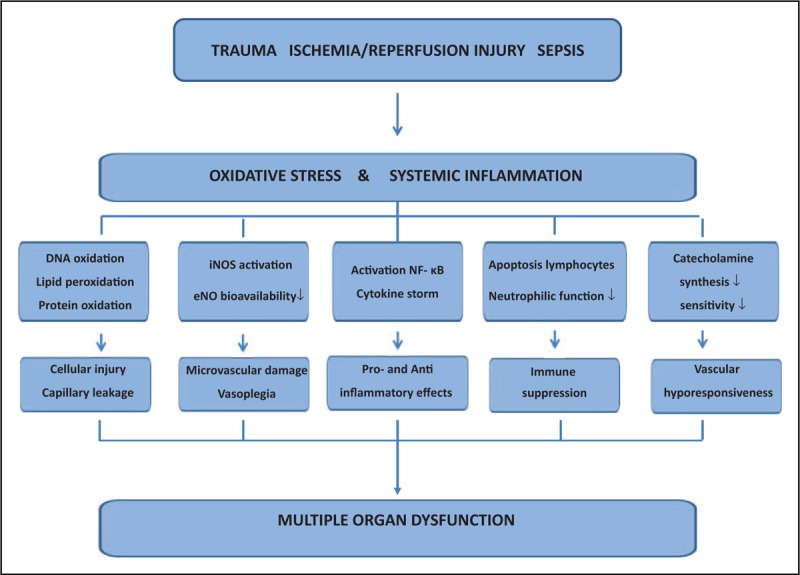
Recent findings: Vitamin C is a key circulating antioxidant with anti-inflammatory and immune-supporting effects, and a cofactor for important mono and dioxygenase enzymes. An increasing number of preclinical studies in trauma, ischemia/reperfusion, and sepsis models show that vitamin C administered at pharmacological doses attenuates oxidative stress and inflammation, and restores endothelial and organ function. Older studies showed less organ dysfunction when vitamin C was administered in repletion dose (2-3 g intravenous vitamin C/day). Recent small controlled studies using pharmacological doses (6-16 g/day) suggest that vitamin C reduces vasopressor support and organ dysfunction, and may even decrease mortality.
Summary: A short course of intravenous vitamin C in pharmacological dose seems a promising, well tolerated, and cheap adjuvant therapy to modulate the overwhelming oxidative stress in severe sepsis, trauma, and reperfusion after ischemia. Large randomized controlled trials are necessary to provide more evidence before wide-scale implementation can be recommended.
Figures
References
-
- Amrein K, Oudemans-van Straaten HM, Berger MM. Vitamin therapy in critically ill patients: focus on thiamine, vitamin C, and vitamin D. Intensive Care Med 2018; doi: 10.1007/s00134-018-5107-y [Epub ahead of print]. - PMC - PubMed
-
A recent high-quality review of the studies in intensive care patients reporting vitamin C plasma levels and the controlled studies on the effect of vitamin C in critically ill patients.
-
- Carr AC, Rosengrave PC, Bayer S, et al. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit Care 2017; 21:300. - PMC - PubMed
-
An important study describing hypovitaminosis C and vitamin C deficiency in critically ill patients.
-
- Rice ME, Lee EJ, Choy Y. High levels of ascorbic acid, not glutathione, in the CNS of anoxia-tolerant reptiles contrasted with levels in anoxia-intolerant species. J Neurochem 1995; 64:1790–1799. - PubMed
-
- Nakano K, Suzuki S. Stress-induced change in tissue levels of ascorbic acid and histamine in rats. J Nutr 1984; 114:1602–1608. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
