

Current Classification and Management of Inflammatory Myopathies
- PMID: 29865091
- PMCID: PMC6004913
- DOI: 10.3233/JND-180308
Current Classification and Management of Inflammatory Myopathies
Abstract
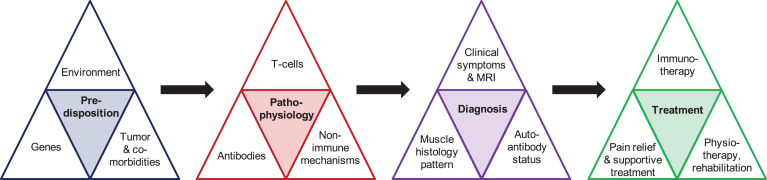
Inflammatory disorders of the skeletal muscle include polymyositis (PM), dermatomyositis (DM), (immune mediated) necrotizing myopathy (NM), overlap syndrome with myositis (overlap myositis, OM) including anti-synthetase syndrome (ASS), and inclusion body myositis (IBM). Whereas DM occurs in children and adults, all other forms of myositis mostly develop in middle aged individuals. Apart from a slowly progressive, chronic disease course in IBM, patients with myositis typically present with a subacute onset of weakness of arms and legs, often associated with pain and clearly elevated creatine kinase in the serum. PM, DM and most patients with NM and OM usually respond to immunosuppressive therapy, whereas IBM is largely refractory to treatment. The diagnosis of myositis requires careful and combinatorial assessment of (1) clinical symptoms including pattern of weakness and paraclinical tests such as MRI of the muscle and electromyography (EMG), (2) broad analysis of auto-antibodies associated with myositis, and (3) detailed histopathological work-up of a skeletal muscle biopsy. This review provides a comprehensive overview of the current classification, diagnostic pathway, treatment regimen and pathomechanistic understanding of myositis.
Keywords: Skeletal muscle; autoimmunity; immunosuppression; muscle inflammation; myositis; neuroinflammation.
Conflict of interest statement
JS has received honoraria, research grants or reimbursements for travel from Bayer, Biogen, BioMarin, Biotest, CSL Behring, Grifols, Hormosan, Novartis, and Octapharma.
Figures
References
-
- Dalakas MCInflammatory muscle diseases. N Engl J Med. 2015;372(18):1734–47. - PubMed
-
- Furst DE, Amato AA, Iorga SR, Gajria K, Fernandes AWEpidemiology of adult idiopathic inflammatory myopathies in a U. S. managed care plan. Muscle Nerve. 2012;45(5):676–83. - PubMed
-
- Senecal JL, Raynauld JP, Troyanov YEditorial: A New Classification of Adult Autoimmune Myositis. Arthritis Rheumatol. 2017;69(5):878–84. - PubMed
-
- van der Meulen MFG, Bronner IM, Hoogendijk JE, Burger H, van Venrooij WJ, Voskuyl AE, et al. Polymyositis - An overdiagnosed entity. Neurology. 2003;61(3):316–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
