

Noninvasive ventilation and respiratory physical therapy reduce exercise-induced bronchospasm and pulmonary inflammation in children with asthma: randomized clinical trial
- PMID: 29865929
- PMCID: PMC5990882
- DOI: 10.1177/1753466618777723
Noninvasive ventilation and respiratory physical therapy reduce exercise-induced bronchospasm and pulmonary inflammation in children with asthma: randomized clinical trial
Abstract
Background: Asthma is characterized by hyperresponsiveness of the airways, and exercise-induced bronchospasm (EIB) is a symptom that limits a large proportion of asthmatic patients, especially children. Continuous positive airway pressure (CPAP) leads to a reduction in the reactivity of the airways. The aim of this study was to evaluate the effect of outpatient treatment with CPAP and bilevel pressure combined with respiratory physical therapy for children and adolescents with asthma following bronchial hyperresponsiveness caused by an exercise bronchoprovocation test.
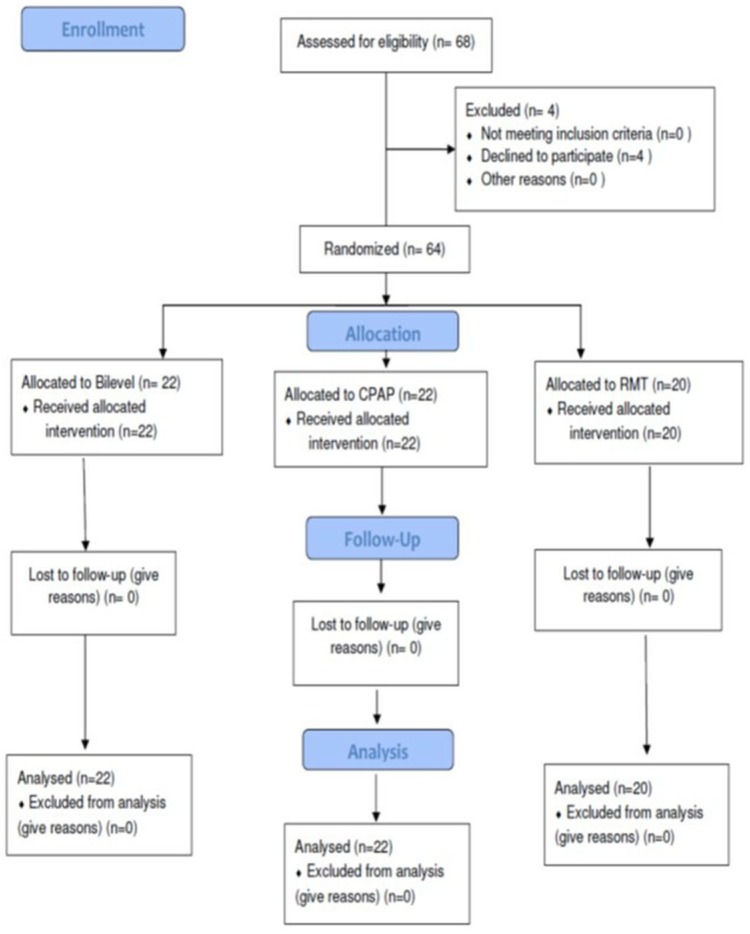
Methods: A randomized, controlled, blind, clinical trial was conducted involving 68 asthmatic children and adolescents aged 4 to 16 years divided into three groups: G1, treated with bilevel pressure (inspiratory positive airway pressure: 12 cm H2O; expiratory positive airway pressure: 8 cm H2O), G2, treated with CPAP (8 cm H2O) and G3, treated with respiratory muscle training (RMT), considered as the control group. All groups were treated at an outpatient clinic and submitted to 10 1-hour sessions, each of which also included respiratory exercises. Evaluations were performed before and after treatment and involved spirometry, an exercise bronchoprovocation test, respiratory pressures, fraction of nitric oxide (FeNO), the Asthma Control Questionnaire (ACQ6) and anthropometric variables. This study received approval from the local ethics committee (certificate number: 1487225/2016) and is registered with ClinicalTrials [ ClinicalTrials.gov identifier: NCT02939625].
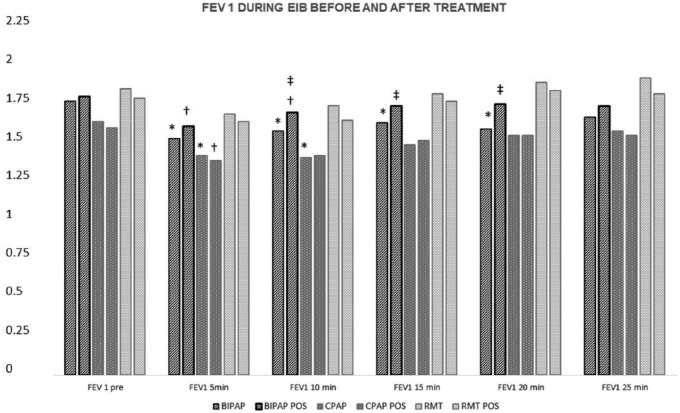
Results: A total of 64 patients concluded the protocol; the mean age of the patients was 10 years. All were in the ideal weight range and had adequate height ( z score: -2 to +2). The three groups demonstrated improved asthma control after the treatments, going from partial to complete control. A significant increase in maximal inspiratory pressure occurred in the three groups, with the greatest increase in the RMT group. A reduction in FeNO in the order of 17.4 parts per billion (effect size: 2.43) and a reduction in bronchial responsiveness on the exercise bronchoprovocation test occurred in the bilevel group. An improvement in FeNO on the order of 15.7 parts per billion (effect size: 2.46) and a reduction in bronchial responsiveness occurred in the CPAP group. No changes in lung function or responsiveness occurred in the RMT group.
Conclusion: Positive pressure and respiratory exercises were effective in reducing pulmonary inflammation, exercise-innduced bronchoespasm (EIB), and increased the clinical control of asthma, as well as RMT, which also resulted in improved clinical control.
Keywords: Asthma; Bilevel; CPAP; EIB; Noninvasive ventilation; asthma control; chest physical therapy; children; lung inflammation; respiratory physical therapy.
Conflict of interest statement
Figures
References
-
- Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) 2018. GINA Report 2018. http://www.ginasthma.org/ (accessed March 2018).
-
- Gleason M, Cicutto L, Haas-Howard C, et al. Leveraging partnerships: families, schools, and providers working together to improve asthma management. Curr Allergy Asthma Rep 2016; 16: 74. - PubMed
-
- McFadden ER, Jr, Ingram RH., Jr Asthma perspectives, definition and classification. In: Fishman AP. (ed) Pulmonary diseases and disorders. New York: McGraw Hill, 1980, pp.562–566.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
