

Patient, family and provider experiences with transfers from intensive care unit to hospital ward: a multicentre qualitative study
- PMID: 29866892
- PMCID: PMC5988518
- DOI: 10.1503/cmaj.170588
Patient, family and provider experiences with transfers from intensive care unit to hospital ward: a multicentre qualitative study
Abstract
Background: Transfer of patient care from an intensive care unit (ICU) to a hospital ward is often challenging, high risk and inefficient. We assessed patient and provider perspectives on barriers and facilitators to high-quality transfers and recommendations to improve the transfer process.
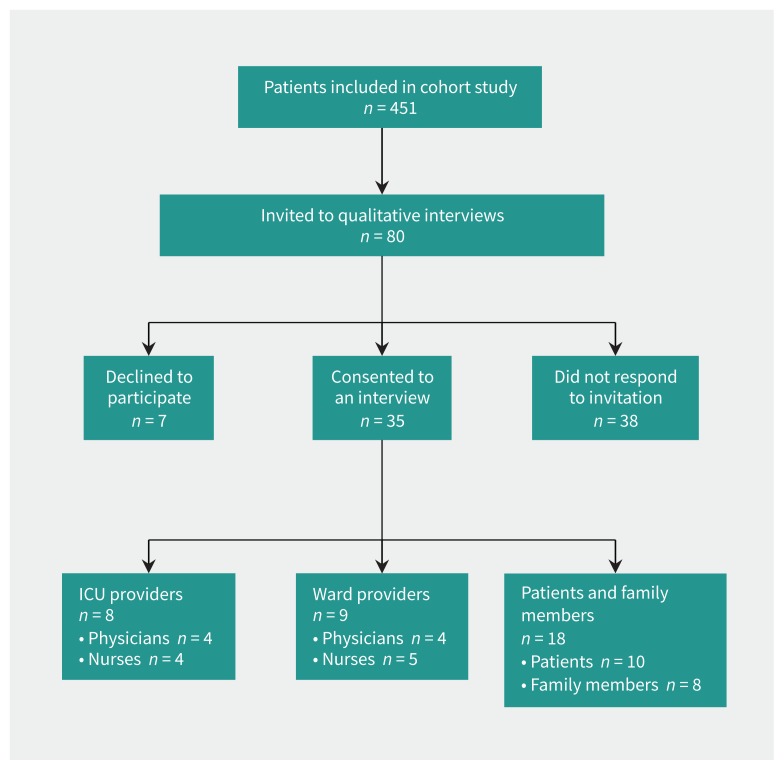
Methods: We conducted semistructured interviews of participants from a multicentre prospective cohort study of ICU transfers conducted at 10 hospitals across Canada. We purposively sampled 1 patient, 1 family member of a patient, 1 ICU provider, and 1 ward provider at each of the 8 English-speaking sites. Qualitative content analysis was used to derive themes, subthemes and recommendations.
Results: The 35 participants described 3 interrelated, overarching themes perceived as barriers or facilitators to high-quality patient transfers: resource availability, communication and institutional culture. Common recommendations suggested to improve ICU transfers included implementing standardized communication tools that streamline provider-provider and provider-patient communication, using multimodal communication to facilitate timely, accurate, durable and mutually reinforcing information transfer; and developing procedures to manage delays in transfer to ensure continuity of care for patients in the ICU waiting for a hospital ward bed.
Interpretation: Patient and provider perspectives attribute breakdown of ICU-to-ward transfers of care to resource availability, communication and institutional culture. Patients and providers recommend standardized, multimodal communication and transfer procedures to improve quality of care.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Sean Bagshaw reports personal fees from Baxter Healthcare, outside the submitted work. No other competing interests were declared.
Figures
References
-
- Singh H, Thomas EJ, Peterson LA, et al. Medical errors involving trainees: a study of closed malpractice claims from 5 insurers. Arch Intern Med 2007; 167:2030–6. - PubMed
-
- Garrouste-Orgeas M, Timsit JF, Vesin A, et al. OUTCOMEREA Study Group. Selected medical errors in the intensive care unit: results of the IATROREF study: parts I and II. Am J Respir Crit Care Med 2010;181:134–42. - PubMed
-
- Naylor M, Brooten D, Jones R, et al. Comprehensive discharge planning for the hospitalized elderly. A randomized clinical trial. Ann Intern Med 1994;120:999–1006. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical