

Metabolic patterns in insulin-resistant male hypogonadism
- PMID: 29867095
- PMCID: PMC5986816
- DOI: 10.1038/s41419-018-0587-9
Metabolic patterns in insulin-resistant male hypogonadism
Abstract
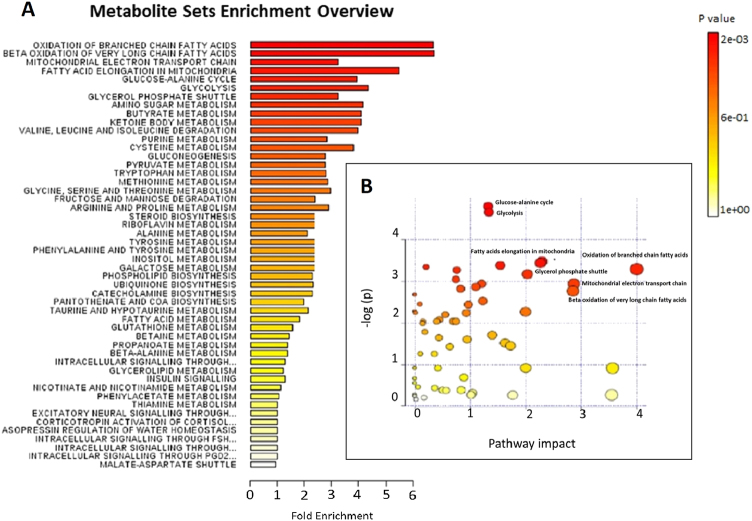
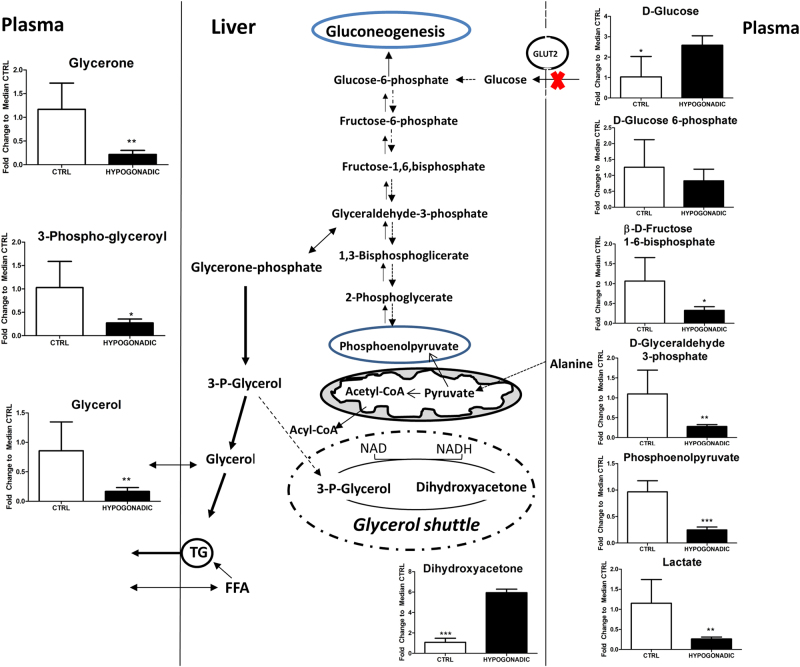
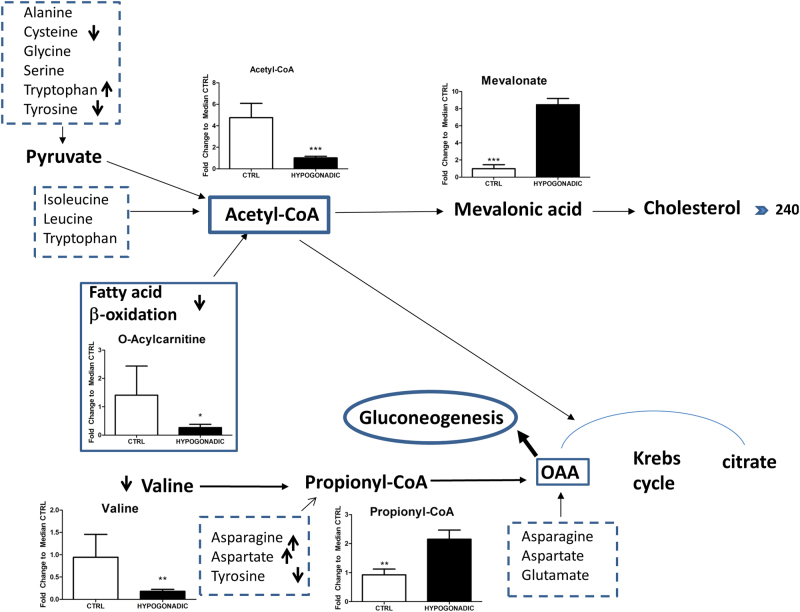
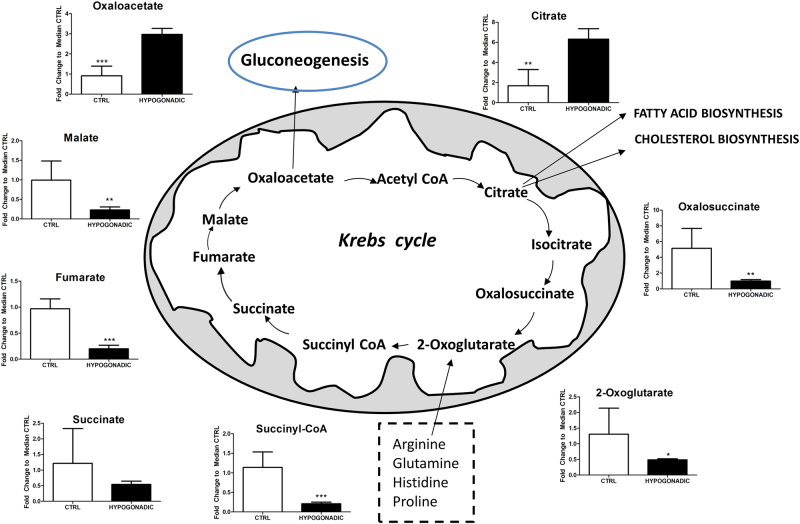
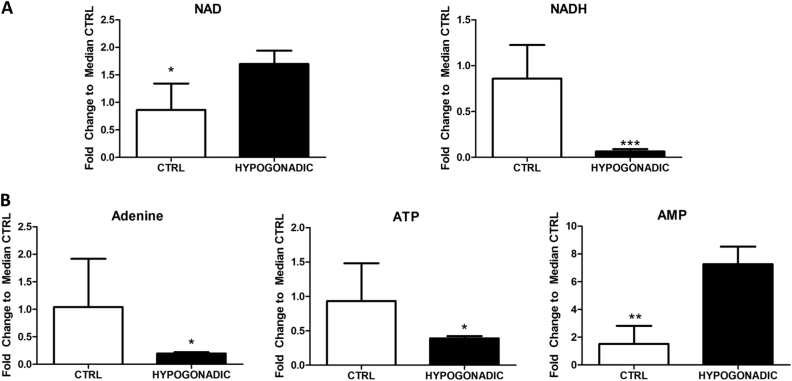
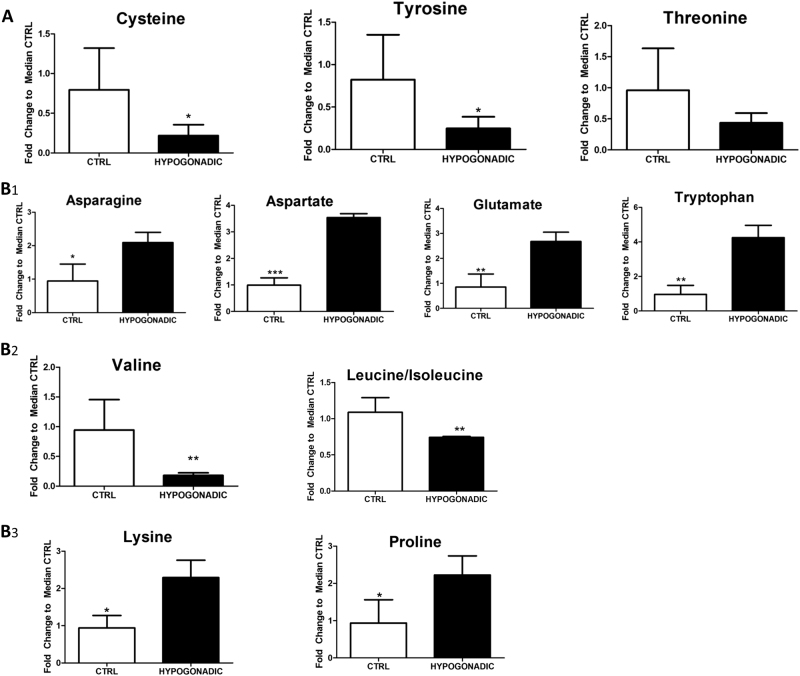
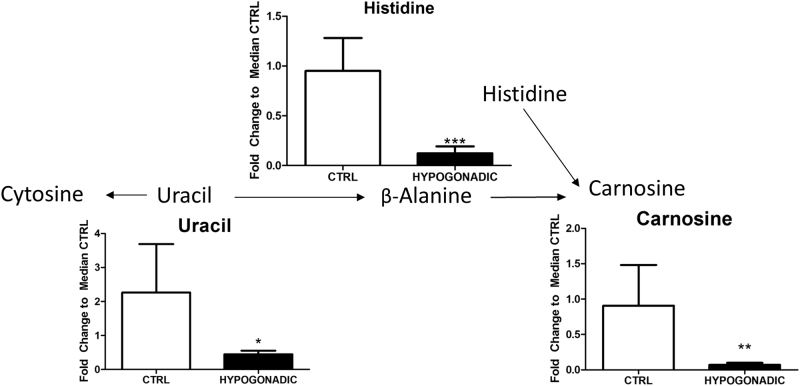
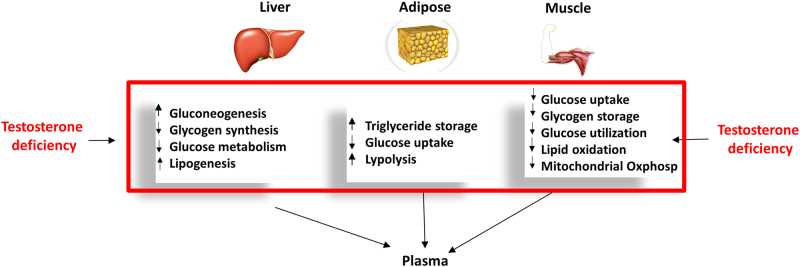
Male hypogonadism associated with insulin resistance (IR) very often leads to metabolic syndrome, at variance with hypogonadism in its first stadium of insulin sensitivity (IS). A plasma metabolomic investigation of these patients can provide useful information in comparison with the values of IS patients. To this aim plasma from insulin-resistant males with hypogonadism were analysed by using ultra high-performance liquid chromatography (UHPLC) and high-resolution mass spectrometry (HRMS). Thus, metabolites were compared to the controls through multivariate statistical analysis and grouped by metabolic pathways. Metabolite database searches and pathway analyses identified imbalances in 18-20 metabolic pathways. Glucose metabolism (e.g., glycolysis and the Krebs cycle) is fuelled by amino acids degradation, in particular of branched amino acids, in individuals with lean body mass. Gluconeogenesis is strongly activated. Some crucial pathways such as glycerol are skewed. Mitochondrial electron transport is affected with a reduction in ATP production. Beta-oxidation of short and medium chain fatty acids did not represent an energy source in hypogonadism, at variance with long and branched fatty acids, justifying the increase in fat mass. Carnosine and β-alanine are strongly reduced resulting in increased fatigue and mental confusion. A comparison of IR with IS male hypogonadism will contribute to a better understanding of how these two hormones work in synergy or antagonise each other in humans. It could also help to select patients who will respond to hormone treatment, and provide accurate biomarkers to measure the response to treatment eventually leading to better strategies in preventing systemic complications in patients not fit for hormone replacement therapy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
