

Universal Pre-Ejection Period Estimation Using Seismocardiography: Quantifying the Effects of Sensor Placement and Regression Algorithms
- PMID: 29867294
- PMCID: PMC5983029
- DOI: 10.1109/jsen.2017.2787628
Universal Pre-Ejection Period Estimation Using Seismocardiography: Quantifying the Effects of Sensor Placement and Regression Algorithms
Abstract
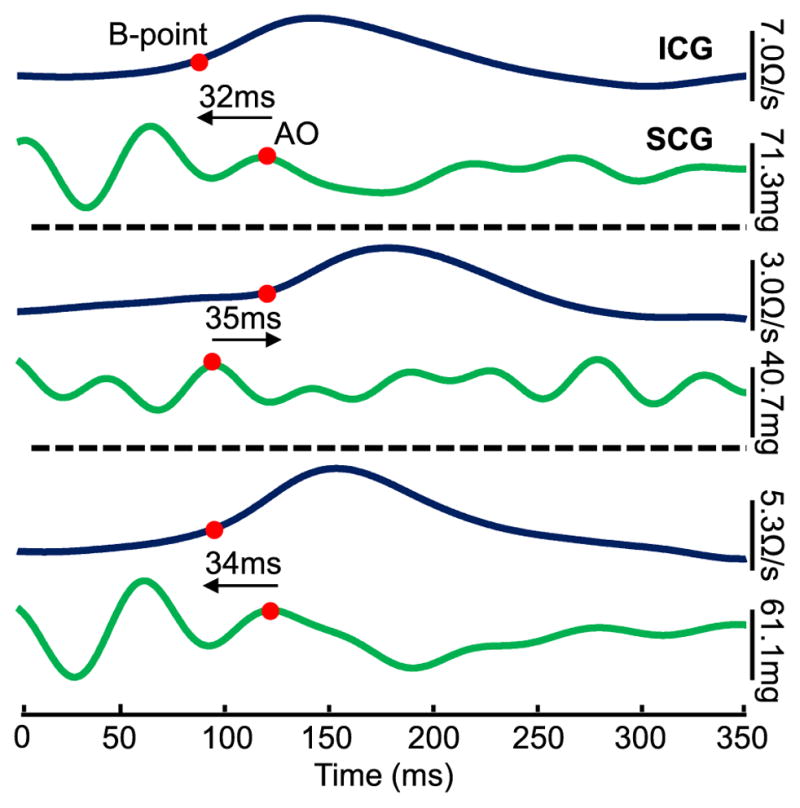
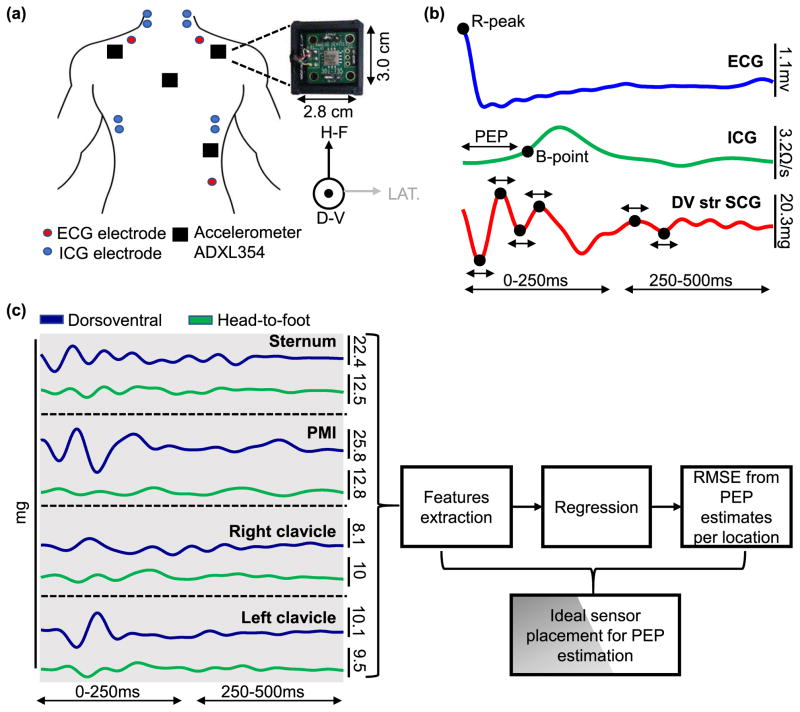
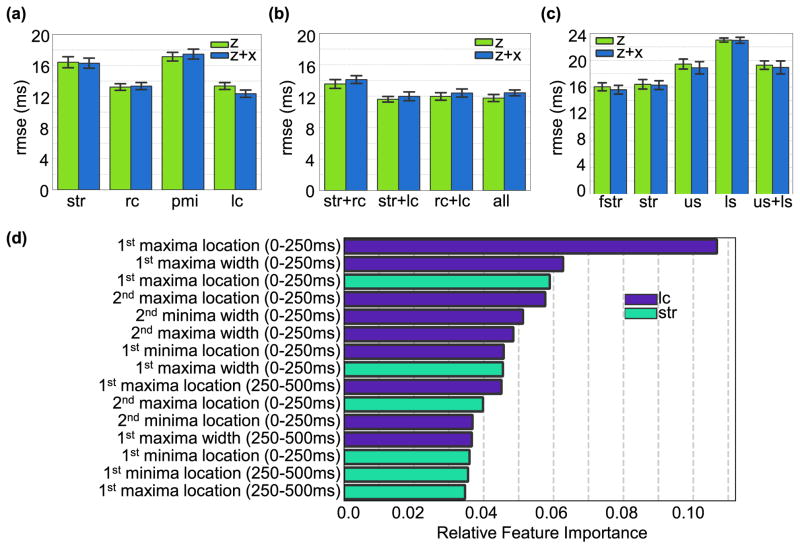
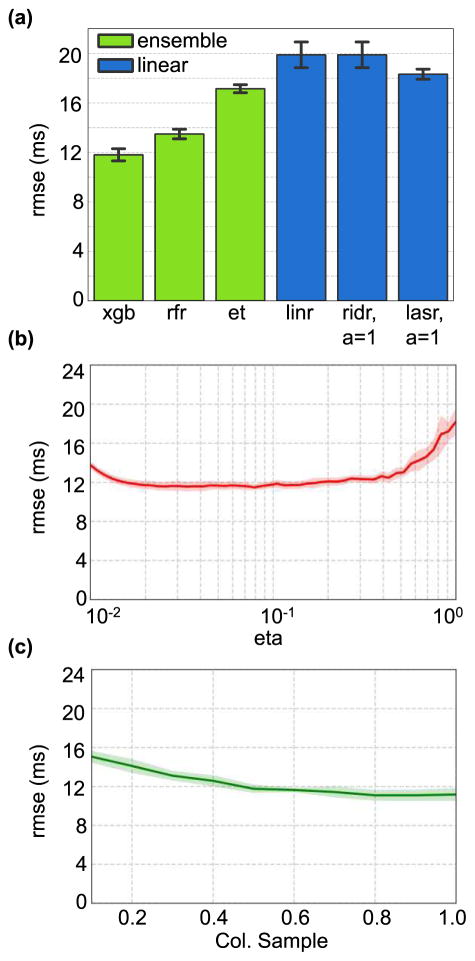
Seismocardiography (SCG), the measurement of local chest vibrations due to the heart and blood movement, is a non-invasive technique to assess cardiac contractility via systolic time intervals such as the pre-ejection period (PEP). Recent studies show that SCG signals measured before and after exercise can effectively classify compensated and decompensated heart failure (HF) patients through PEP estimation. However, the morphology of the SCG signal varies from person to person and sensor placement making it difficult to automatically estimate PEP from SCG and electrocardiogram signals using a global model. In this proof-of-concept study, we address this problem by extracting a set of timing features from SCG signals measured from multiple positions on the upper body. We then test global regression models that combine all the detected features to identify the most accurate model for PEP estimation obtained from the best performing regressor and the best sensor location or combination of locations. Our results show that ensemble regression using XGBoost with a combination of sensors placed on the sternum and below the left clavicle provide the best RMSE = 11.6 ± 0.4 ms across all subjects. We also show that placing the sensor below the left or right clavicle rather than the conventional placement on the sternum results in more accurate PEP estimates.
Keywords: Seismocardiogram; accelerometer; ensemble regression; heart failure; pre-ejection period; sensor fusion; unobtrusive cardiovascular monitoring.
Figures
References
-
- Katz AM. Physiology of the heart. New York: Raven Press; 1977. p. xiii.p. 450.
-
- Heidenreich PA, et al. Forecasting the future of cardiovascular disease in the United States. Circulation. 2011;123(8):933–944. - PubMed
-
- Inan OT, et al. Using Ballistocardiography to Monitor Left Ventricular Function in Heart Failure Patients. Journal of Cardiac Failure. 2016;22(8):S45.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous