

Validated Computational Model to Compute Re-apposition Pressures for Treating Type-B Aortic Dissections
- PMID: 29867557
- PMCID: PMC5954206
- DOI: 10.3389/fphys.2018.00513
Validated Computational Model to Compute Re-apposition Pressures for Treating Type-B Aortic Dissections
Abstract
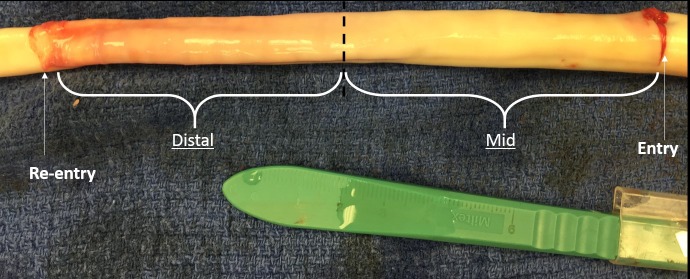
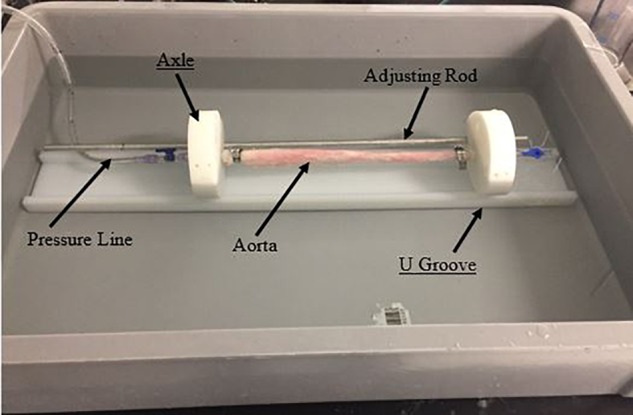
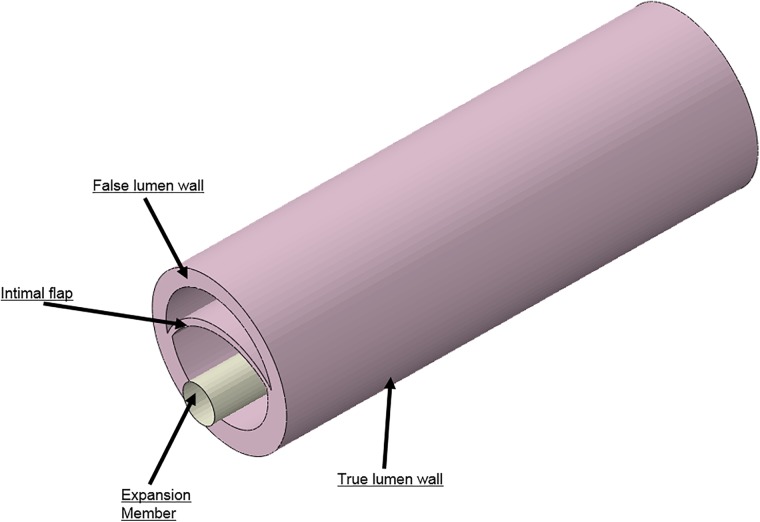
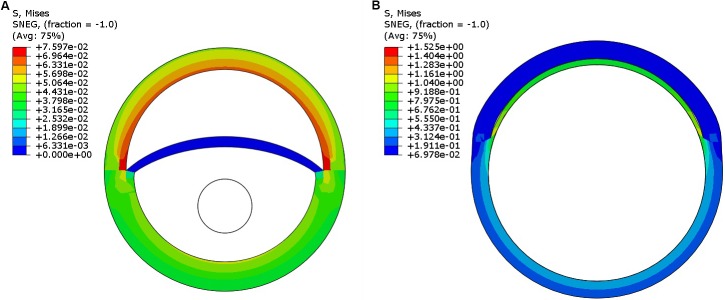
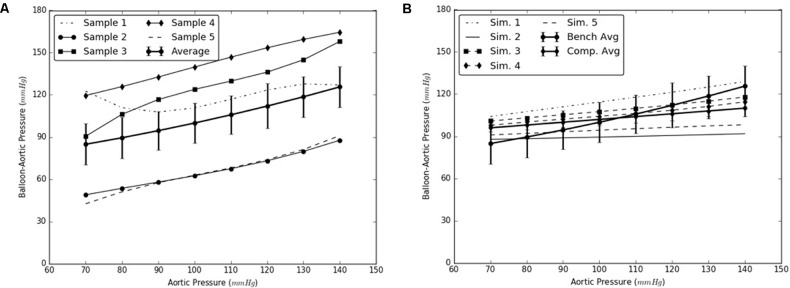
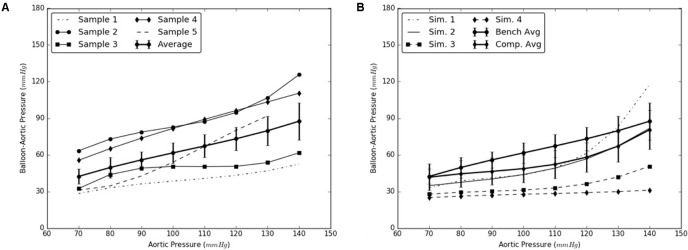
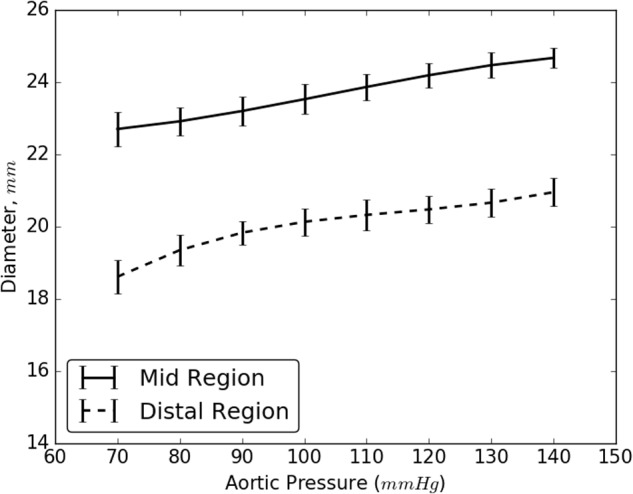
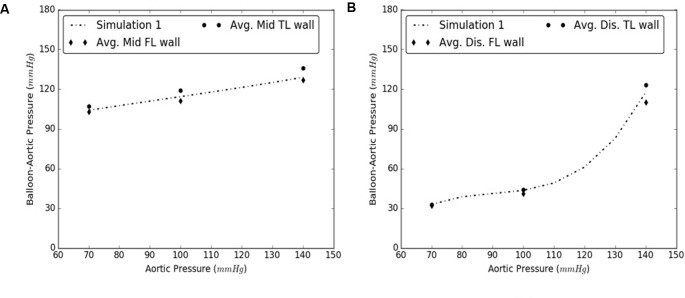
The use of endovascular treatment in the thoracic aorta has revolutionized the clinical approach for treating Stanford type B aortic dissection. The endograft procedure is a minimally invasive alternative to traditional surgery for the management of complicated type-B patients. The endograft is first deployed to exclude the proximal entry tear to redirect blood flow toward the true lumen and then a stent graft is used to push the intimal flap against the false lumen (FL) wall such that the aorta is reconstituted by sealing the FL. Although endovascular treatment has reduced the mortality rate in patients compared to those undergoing surgical repair, more than 30% of patients who were initially successfully treated require a new endovascular or surgical intervention in the aortic segments distal to the endograft. One reason for failure of the repair is persistent FL perfusion from distal entry tears. This creates a patent FL channel which can be associated with FL growth. Thus, it is necessary to develop stents that can promote full re-apposition of the flap leading to complete closure of the FL. In the current study, we determine the radial pressures required to re-appose the mid and distal ends of a dissected porcine thoracic aorta using a balloon catheter under static inflation pressure. The same analysis is simulated using finite element analysis (FEA) models by incorporating the hyperelastic properties of porcine aortic tissues. It is shown that the FEA models capture the change in the radial pressures required to re-appose the intimal flap as a function of pressure. The predictions from the simulation models match closely the results from the bench experiments. The use of validated computational models can support development of better stents by calculating the proper radial pressures required for complete re-apposition of the intimal flap.
Keywords: aortic dissection; bench tests; finite element analysis; porcine aorta; re-apposition pressure; simulation models.
Figures


References
-
- Andersen N. D., Keenan J. E., Ganapathi A. M., Gaca J. G., McCann R. L., Hughes G. C. (2014). Current management and outcome of chronic type B aortic dissection: results with open and endovascular repair since the advent of thoracic endografting. 3 264–274. 10.3978/j.issn.2225-319X.2014.05.07 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources