

Pancreatic Ductal Adenocarcinoma: A Strong Imbalance of Good and Bad Immunological Cops in the Tumor Microenvironment
- PMID: 29868007
- PMCID: PMC5960705
- DOI: 10.3389/fimmu.2018.01044
Pancreatic Ductal Adenocarcinoma: A Strong Imbalance of Good and Bad Immunological Cops in the Tumor Microenvironment
Abstract
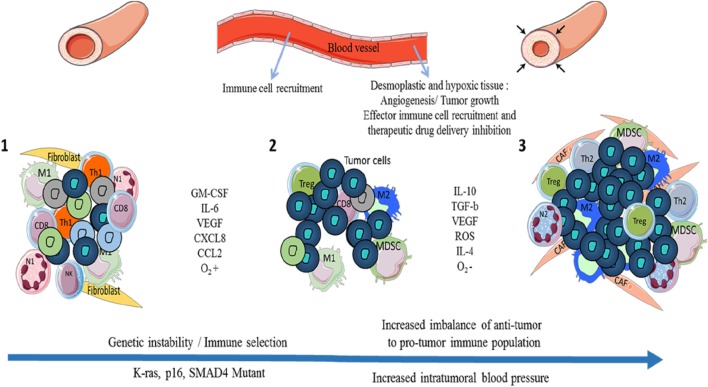
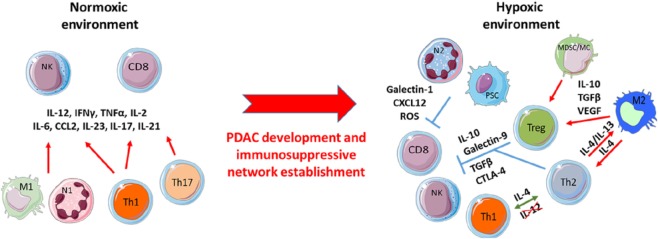
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive and lethal cancers with very few available treatments. For many decades, gemcitabine was the only treatment for patients with PDAC. A recent attempt to improve patient survival by combining this chemotherapy with FOLFIRINOX and nab-paclitaxel failed and instead resulted in increased toxicity. Novel therapies are urgently required to improve PDAC patient survival. New treatments in other cancers such as melanoma, non-small-cell lung cancer, and renal cancer have emerged, based on immunotherapy targeting the immune checkpoints cytotoxic T-lymphocyte-associated antigen 4 or programmed death 1 ligand. However, the first clinical trials using such immune checkpoint inhibitors in PDAC have had limited success. Resistance to immunotherapy in PDAC remains unclear but could be due to tissue components (cancer-associated fibroblasts, desmoplasia, hypoxia) and to the imbalance between immunosuppressive and effector immune populations in the tumor microenvironment. In this review, we analyzed the presence of "good and bad immunological cops" in PDAC and discussed the significance of changes in their balance.
Keywords: hypoxia; immune checkpoint; immune infiltrate; immunosuppression; pancreatic ductal adenocarcinoma; tumor microenvironment.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials