

The Arthroscopic Bankart-Plus Procedure for Treatment of Anterior Shoulder Instability With Small to Intermediate Glenoid Defects
- PMID: 29868408
- PMCID: PMC5982609
- DOI: 10.1016/j.eats.2017.10.009
The Arthroscopic Bankart-Plus Procedure for Treatment of Anterior Shoulder Instability With Small to Intermediate Glenoid Defects
Abstract
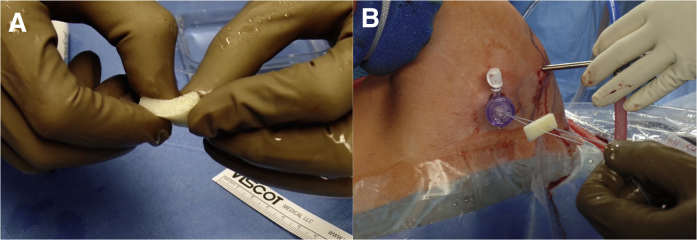
To date, specific surgical procedures are available for the treatment of anterior shoulder instability with substantial bony glenoid defects, as well as for patients without osseous lesions. However, specific treatment options are lacking for the frequently observed small to intermediate glenoid defects, which may not necessitate glenoid reconstruction surgery according to current guidelines but can still jeopardize the outcome after mere soft-tissue stabilization procedures. This article describes the so-called arthroscopic Bankart-Plus procedure for the treatment of anterior shoulder instability with small to intermediate bony glenoid defects. In addition to the conventional capsulolabral repair, an allogeneic demineralized spongy bone matrix is inserted between the glenoid neck and the labrum with the aim of compensating for the glenoid bone loss by increasing the volume of the labrum and thus its stabilizing effect.
Figures



References
-
- Griffith J.F., Antonio G.E., Yung P.S. Prevalence, pattern, and spectrum of glenoid bone loss in anterior shoulder dislocation: CT analysis of 218 patients. AJR Am J Roentgenol. 2008;190:1247–1254. - PubMed
-
- Yamamoto N., Muraki T., Sperling J.W. Stabilizing mechanism in bone-grafting of a large glenoid defect. J Bone Joint Surg Am. 2010;92:2059–2066. - PubMed
-
- Burkhart S.S., De Beer J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677–694. - PubMed
-
- Bushnell B.D., Creighton R.A., Herring M.M. Bony instability of the shoulder. Arthroscopy. 2008;24:1061–1073. - PubMed
-
- Shaha J.S., Cook J.B., Song D.J. Redefining “critical” bone loss in shoulder instability: Functional outcomes worsen with “subcritical” bone loss. Am J Sports Med. 2015;43:1719–1725. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
