

Normalization of Soluble CD163 Levels After Institution of Antiretroviral Therapy During Acute HIV Infection Tracks with Fewer Neurological Abnormalities
- PMID: 29868826
- PMCID: PMC6151077
- DOI: 10.1093/infdis/jiy337
Normalization of Soluble CD163 Levels After Institution of Antiretroviral Therapy During Acute HIV Infection Tracks with Fewer Neurological Abnormalities
Abstract
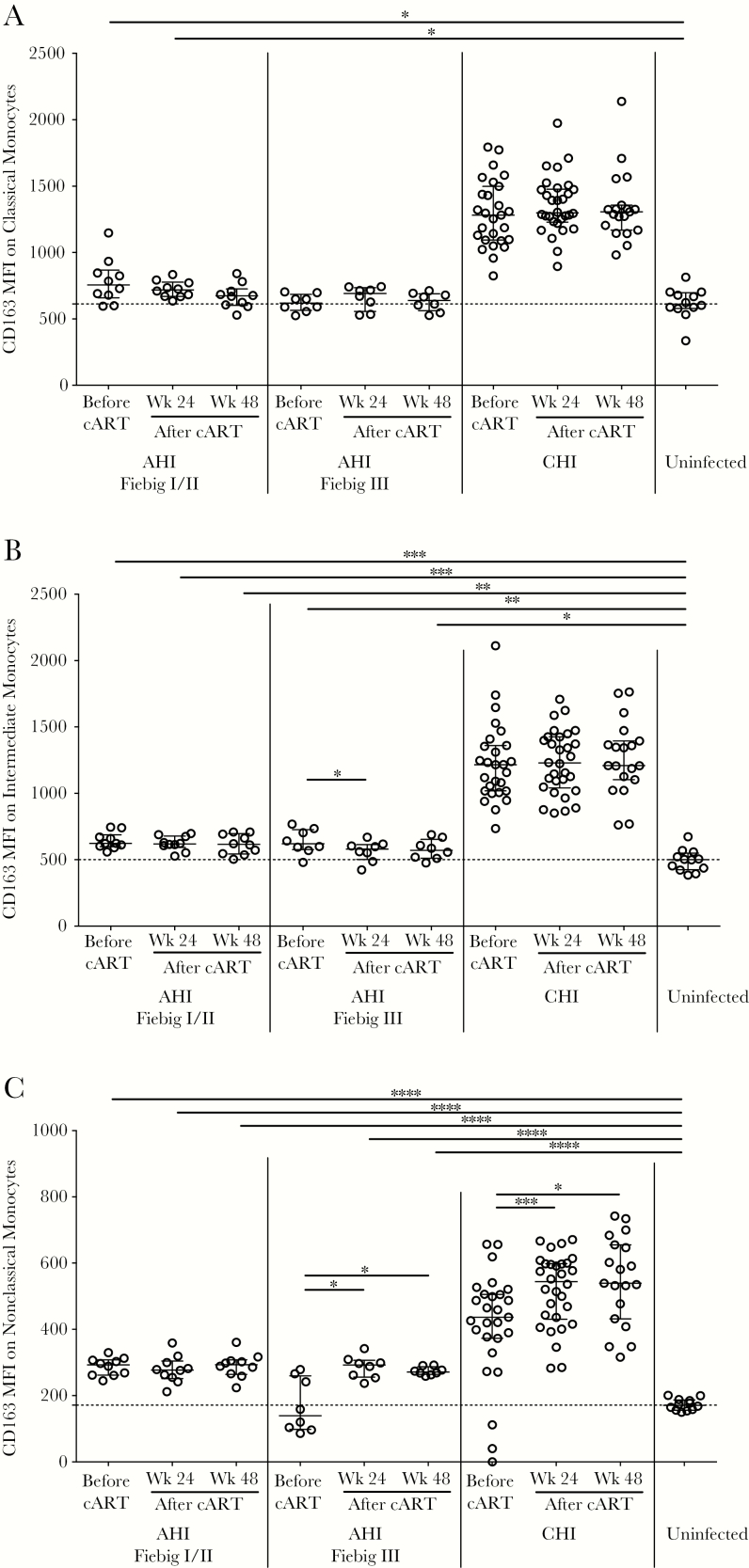
Background: Myeloid activation contributes to cognitive impairment in chronic human immunodeficiency virus (HIV) infection. We explored whether combination antiretroviral therapy (cART) initiation during acute HIV infection impacts CD163 shedding, a myeloid activation marker, and in turn, implications on the central nervous system (CNS).
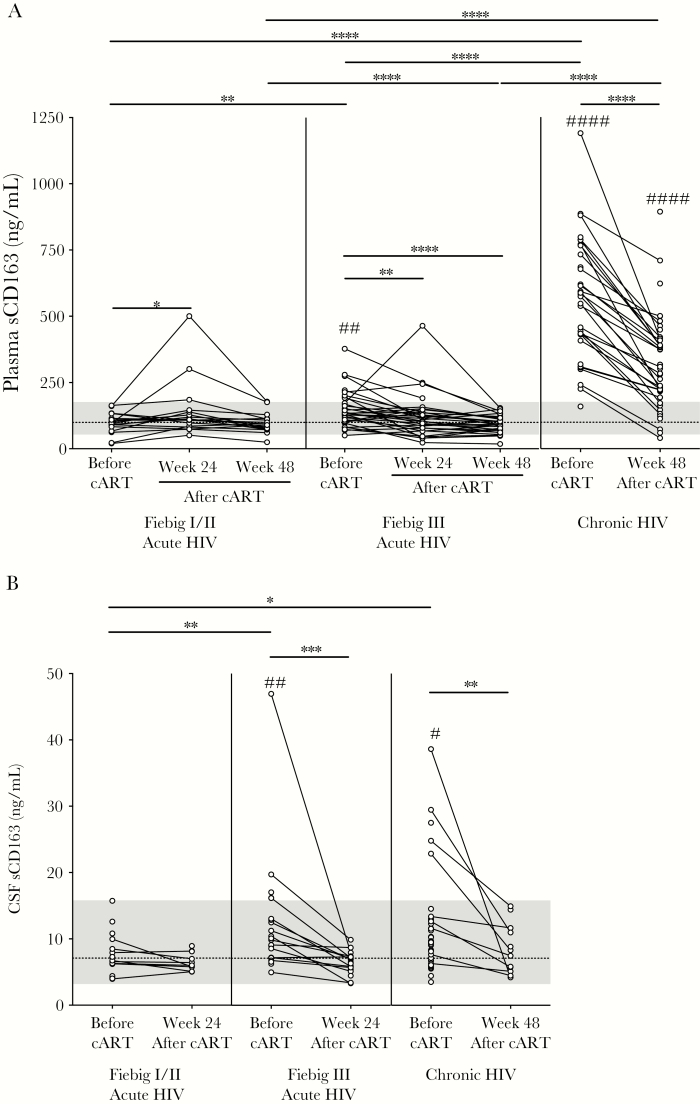
Methods: We measured soluble CD163 (sCD163) levels in plasma and cerebrospinal fluid (CSF) by enzyme-linked immunosorbent assay in Thais who initiated cART during acute HIV infection (Fiebig stages I-IV). Examination of CNS involvement included neuropsychological testing and analysis of brain metabolites by magnetic resonance spectroscopy. Chronic HIV-infected or uninfected Thais served as controls.
Results: We examined 51 adults with acute HIV infection (Fiebig stages I-III; male sex, >90%; age, 31 years). sCD163 levels before and after cART in Fiebig stage I/II were comparable to those in uninfected controls (plasma levels, 97.9 and 93.6 ng/mL, respectively, vs 99.5 ng/mL; CSF levels, 6.7 and 6.4 ng/mL, respectively, vs 7.1 ng/mL). In Fiebig stage III, sCD163 levels were elevated before cART as compared to those in uninfected controls (plasma levels, 135 ng/mL; CSF levels, 10 ng/mL; P < .01 for both comparisons) before normalization after cART (plasma levels, 90.1 ng/mL; CSF levels, 6.5 ng/mL). Before cART, higher sCD163 levels during Fiebig stage III correlated with poor CNS measures (eg, decreased N-acetylaspartate levels), but paradoxically, during Fiebig stage I/II, this association was linked with favorable CNS outcomes (eg, higher neuropsychological test scores). After cART initiation, higher sCD163 levels during Fiebig stage III were associated with negative CNS indices (eg, worse neuropsychological test scores).
Conclusion: Initiation of cART early during acute HIV infection (ie, during Fiebig stage I/II) may decrease inflammation, preventing shedding of CD163, which in turn might lower the risk of brain injury.
Figures
References
-
- Tozzi V, Balestra P, Salvatori MF, et al. . Changes in cognition during antiretroviral therapy: comparison of 2 different ranking systems to measure antiretroviral drug efficacy on HIV-associated neurocognitive disorders. J Acquir Immune Defic Syndr 2009; 52:56–63. - PubMed
-
- Sereti I, Krebs SJ, Phanuphak N, et al. . Initiation of antiretroviral therapy in early HIV infection reduces but does not abrogate chronic residual inflammation. Clin Infect Dis 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
