

Validating the use of bioimpedance spectroscopy for assessment of fluid status in children
- PMID: 29869117
- PMCID: PMC6061658
- DOI: 10.1007/s00467-018-3971-x
Validating the use of bioimpedance spectroscopy for assessment of fluid status in children
Abstract
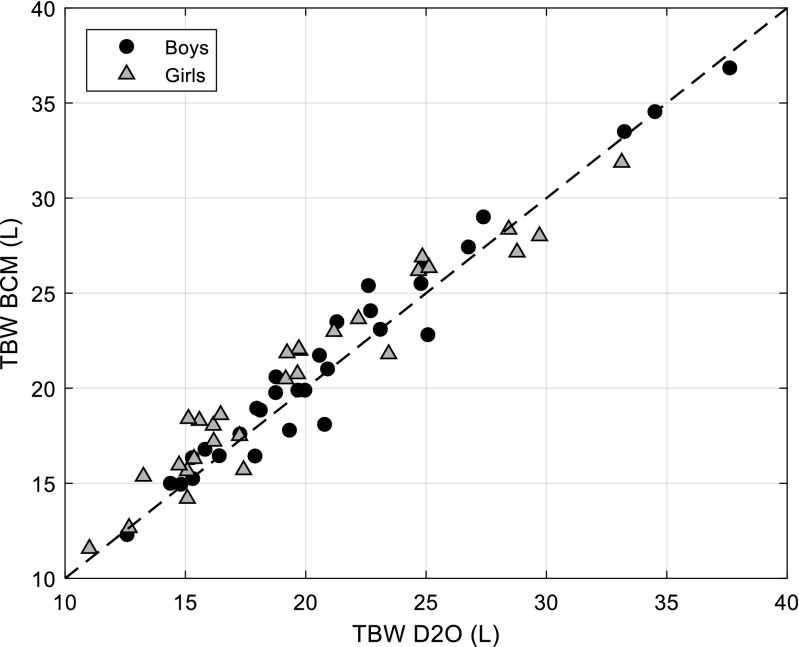
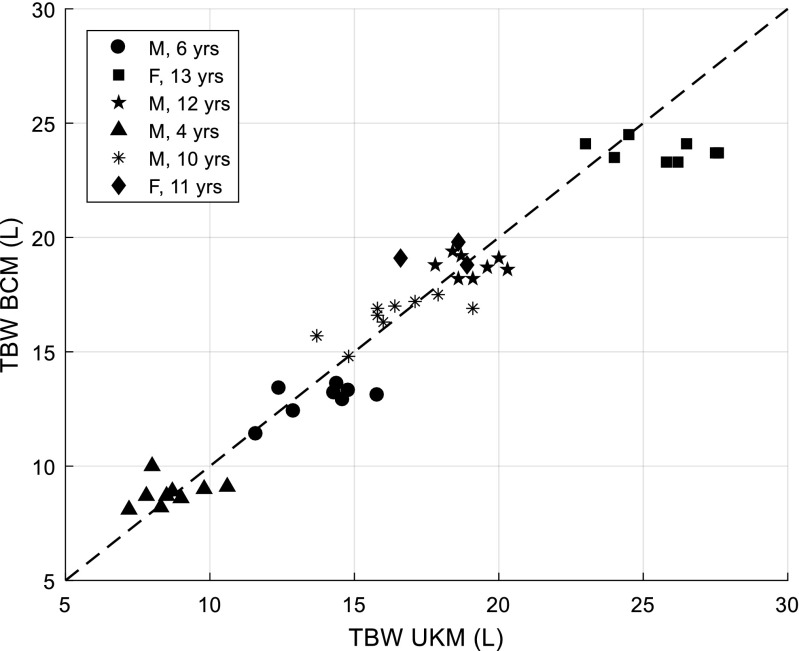
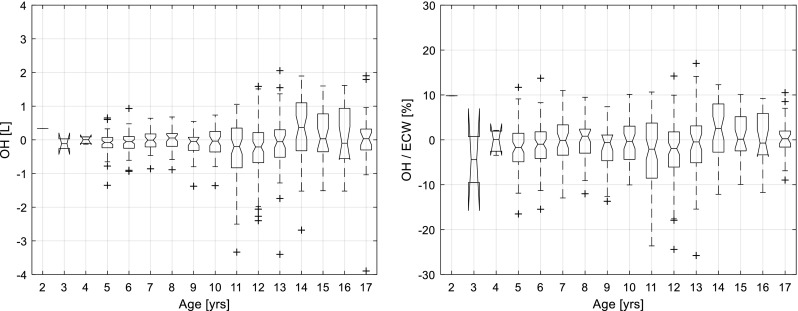
Background: Bioimpedance spectroscopy (BIS) with a whole-body model to distinguish excess fluid from major body tissue hydration can provide objective assessment of fluid status. BIS is integrated into the Body Composition Monitor (BCM) and is validated in adults, but not children. This study aimed to (1) assess agreement between BCM-measured total body water (TBW) and a gold standard technique in healthy children, (2) compare TBW_BCM with TBW from Urea Kinetic Modelling (UKM) in haemodialysis children and (3) investigate systematic deviation from zero in measured excess fluid in healthy children across paediatric age range.
Methods: TBW_BCM and excess fluid was determined from standard wrist-to-ankle BCM measurement. TBW_D2O was determined from deuterium concentration decline in serial urine samples over 5 days in healthy children. UKM was used to measure body water in children receiving haemodialysis. Agreement between methods was analysed using paired t test and Bland-Altman method comparison.
Results: In 61 healthy children (6-14 years, 32 male), mean TBW_BCM and TBW_D2O were 21.1 ± 5.6 and 20.5 ± 5.8 L respectively. There was good agreement between TBW_BCM and TBW_D2O (R2 = 0.97). In six haemodialysis children (4-13 years, 4 male), 45 concomitant measurements over 8 months showed good TBW_BCM and TBW_UKM agreement (mean difference - 0.4 L, 2SD = ± 3.0 L). In 634 healthy children (2-17 years, 300 male), BCM-measured overhydration was - 0.1 ± 0.7 L (10-90th percentile - 0.8 to + 0.6 L). There was no correlation between age and OH (p = 0.28).
Conclusions: These results suggest BCM can be used in children as young as 2 years to measure normally hydrated weight and assess fluid status.
Keywords: Bioimpedance; Children; Chronic kidney disease; Fluid volume; Haemodialysis; Overhydration; Total body water.
Conflict of interest statement
EL received honoraria from Fresenius Medical Care for providing training in the use of bioimpedance spectroscopy in renal care.
PC, PW and UM are employees of Fresenius Medical Care.
Figures
Comment in
-
Total body water measurement in childhood.Pediatr Nephrol. 2019 Jan;34(1):183. doi: 10.1007/s00467-018-4077-1. Epub 2018 Sep 20. Pediatr Nephrol. 2019. PMID: 30238150 No abstract available.
-
Even gold standard methods of body water measurement are not always in perfect agreement.Pediatr Nephrol. 2019 Jan;34(1):185-186. doi: 10.1007/s00467-018-4089-x. Epub 2018 Oct 1. Pediatr Nephrol. 2019. PMID: 30276535 No abstract available.
References
-
- Hecking M, Karaboyas A, Antlanger M, Saran R, Wizemann V, Chazot C, Rayner H, Hörl WH, Pisoni RL, Robinson BM, Sunder-Plassmann G, Moissl U. Significance of interdialytic weight gain versus chronic volume overload: consensus opinion. Am J Nephrol. 2013;38:78–90. doi: 10.1159/000353104. - DOI - PubMed
-
- Weiner DE, Brunelli SM, Hunt A, Schiller B, Glassock R, Maddux FW, Johnson D, Parker T, Nissenson A. Improving clinical outcomes among hemodialysis patients: a proposal for a “volume first” approach from the chief medical officers of US dialysis providers. Am J Kidney Dis. 2014;64:685–695. doi: 10.1053/j.ajkd.2014.07.003. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
