

Corneal confocal microscopy for identification of diabetic sensorimotor polyneuropathy: a pooled multinational consortium study
- PMID: 29869146
- PMCID: PMC6061173
- DOI: 10.1007/s00125-018-4653-8
Corneal confocal microscopy for identification of diabetic sensorimotor polyneuropathy: a pooled multinational consortium study
Abstract
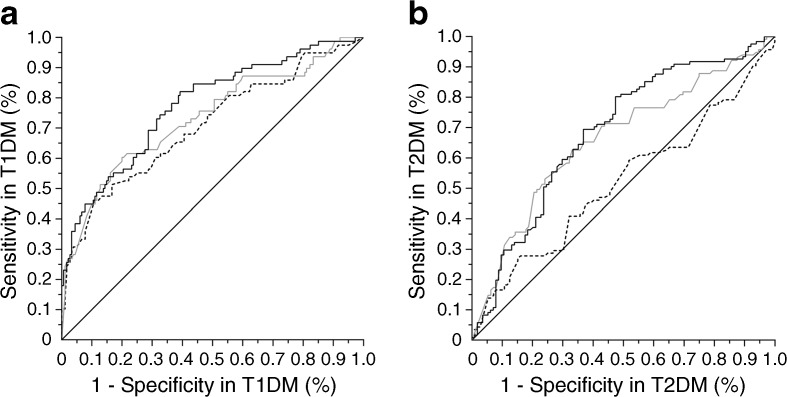
Aims/hypothesis: Small cohort studies raise the hypothesis that corneal nerve abnormalities (including corneal nerve fibre length [CNFL]) are valid non-invasive imaging endpoints for diabetic sensorimotor polyneuropathy (DSP). We aimed to establish concurrent validity and diagnostic thresholds in a large cohort of participants with and without DSP.
Methods: Nine hundred and ninety-eight participants from five centres (516 with type 1 diabetes and 482 with type 2 diabetes) underwent CNFL quantification and clinical and electrophysiological examination. AUC and diagnostic thresholds were derived and validated in randomly selected samples using receiver operating characteristic analysis. Sensitivity analyses included latent class models to address the issue of imperfect reference standard.
Results: Type 1 and type 2 diabetes subcohorts had mean age of 42 ± 19 and 62 ± 10 years, diabetes duration 21 ± 15 and 12 ± 9 years and DSP prevalence of 31% and 53%, respectively. Derivation AUC for CNFL was 0.77 in type 1 diabetes (p < 0.001) and 0.68 in type 2 diabetes (p < 0.001) and was approximately reproduced in validation sets. The optimal threshold for automated CNFL was 12.5 mm/mm2 in type 1 diabetes and 12.3 mm/mm2 in type 2 diabetes. In the total cohort, a lower threshold value below 8.6 mm/mm2 to rule in DSP and an upper value of 15.3 mm/mm2 to rule out DSP were associated with 88% specificity and 88% sensitivity.
Conclusions/interpretation: We established the diagnostic validity and common diagnostic thresholds for CNFL in type 1 and type 2 diabetes. Further research must determine to what extent CNFL can be deployed in clinical practice and in clinical trials assessing the efficacy of disease-modifying therapies for DSP.
Keywords: Corneal confocal microscopy; Corneal nerves; Diabetic neuropathy; Diabetic sensorimotor polyneuropathy; Small nerve fibre morphology.
Conflict of interest statement
BAP reports grants from CIHR, NIH and JDRF, speaker honoraria from Medtronic, Johnson & Johnson, Insulet, Abbott, Novo Nordisk and Sanofi and research grant support from Medtronic and Boehringer Ingelheim and serves as a consultant for Boehringer Ingelheim, Insulet and Novo Nordisk. NE reports grants from JDRF and NHMRC during the conduct of the study. DP reports grants from NIH RFA DK-13-027 and grants from JDRF during the conduct of the study. JKM has received research grants from Eli Lilly, Pfizer, Bristol-Myers Squibb, PTC Therapeutics, Sanofi Genzyme, Novartis, ReveraGen Pharma and Biogen. SIL reports grants from NIH-DHHS-US through a consortium with Mount Sinai Hospital and grants from NIH-NIDDK Michigan Diabetes Research Center Diabetes Interdisciplinary Study Grant during the conduct of the study. All other authors declare that there is no duality of interest associated with their contribution to this manuscript.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
