

Obsessive-compulsive personality disorder features and response to behavioral therapy for insomnia among patients with hypnotic-dependent insomnia
- PMID: 29869891
- PMCID: PMC6281779
- DOI: 10.1080/15402002.2018.1483369
Obsessive-compulsive personality disorder features and response to behavioral therapy for insomnia among patients with hypnotic-dependent insomnia
Abstract
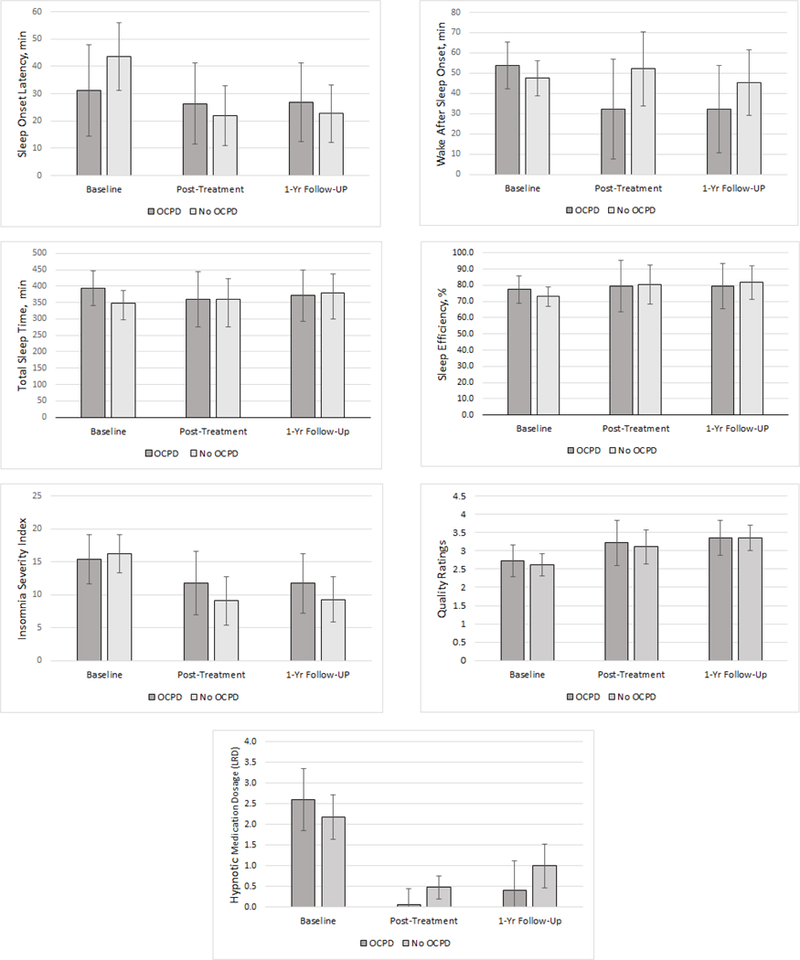
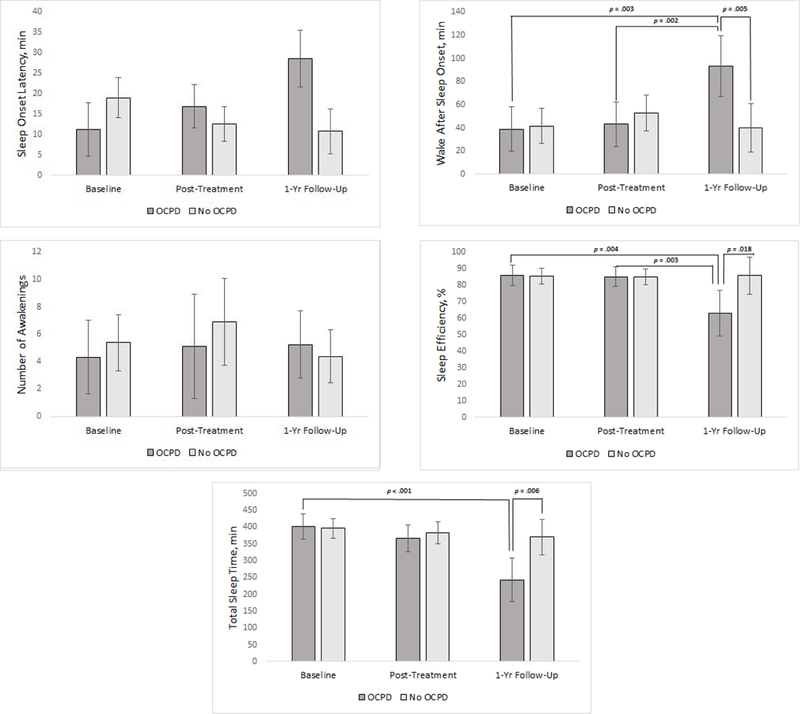
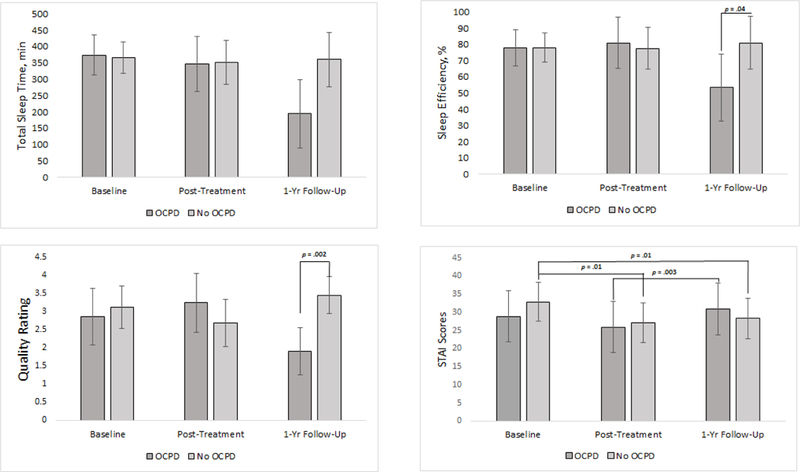
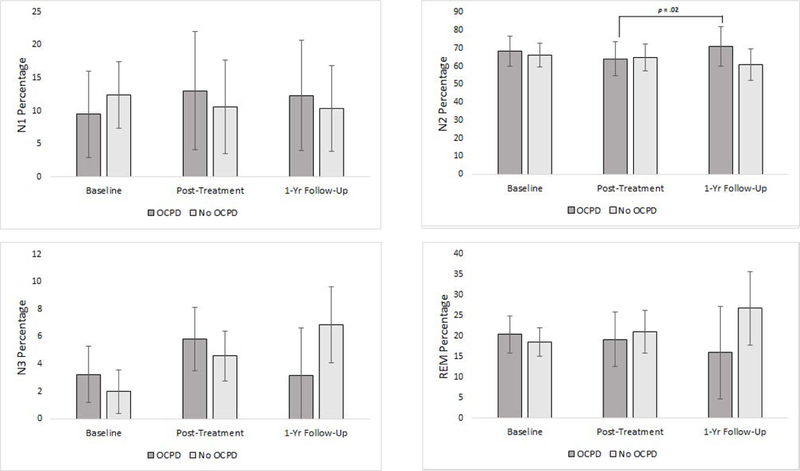
Objective: To compare therapeutic response to behavioral therapy for insomnia (BT-I) among hypnotic-dependent insomnia (HDI) patients with and without Cluster C personality disorders. Participants: Twenty-three adults with HDI (17 females), aged between 33 and 68 (M = 53; SD = 9.9) were included in the study. Methods: Participants completed a personality disorder assessment (baseline), as well as sleep diaries, polysomnography (PSG), and an insomnia severity assessment (baseline, posttreatment, and one-year follow-up). Treatment consisted of eight weeks of individual BT-I and gradual hypnotic medication withdrawal. Multilevel mixed-effects linear regression models examined the interaction between study visit and Cluster C personality disorders status on treatment response to BT-I. Results: Obsessive-compulsive personality disorder (OCPD) was the most prevalent of the Cluster C personality disorders with 38% (n = 8) of participants meeting criteria. There were no significant treatment differences by OCPD status across time as measured by sleep diaries and insomnia severity status. However, there were significant treatment differences by OCPD status by one-year follow-up on PSG outcomes, indicating that patients with OCPD status had shorter and more disrupted sleep than patients without OCPD status. Conclusions: Based on self-reported sleep measures, patients with insomnia and features of OCPD responded equivalently to BT-I at one-year follow-up compared to patients without features of OCPD. However, polysomnography outcomes indicated objective sleep deteriorated in these patients, which may suggest greater vulnerability to relapse.
Figures
Similar articles
-
Personality disorder features and insomnia status amongst hypnotic-dependent adults.Sleep Med. 2012 Oct;13(9):1122-9. doi: 10.1016/j.sleep.2012.05.004. Epub 2012 Aug 28. Sleep Med. 2012. PMID: 22938862 Free PMC article.
-
Psychological treatment of hypnotic-dependent insomnia in a primarily older adult sample.Behav Res Ther. 2013 Dec;51(12):787-96. doi: 10.1016/j.brat.2013.09.006. Epub 2013 Sep 26. Behav Res Ther. 2013. PMID: 24121096 Free PMC article. Clinical Trial.
-
The association between obsessive compulsive disorder and obsessive compulsive personality disorder: prevalence and clinical presentation.Br J Clin Psychol. 2013 Sep;52(3):300-15. doi: 10.1111/bjc.12016. Epub 2013 Jan 18. Br J Clin Psychol. 2013. PMID: 23865406
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.Health Technol Assess. 2004 Feb;8(8):iii-iv, 1-68. doi: 10.3310/hta8080. Health Technol Assess. 2004. PMID: 14960254 Review.
-
Hypnotic Discontinuation in Chronic Insomnia.Sleep Med Clin. 2018 Jun;13(2):263-270. doi: 10.1016/j.jsmc.2018.02.008. Sleep Med Clin. 2018. PMID: 29759276 Review.
Cited by
-
Prevalence of Comorbid Personality Disorder in Psychotic and Non-psychotic Disorders.Front Psychiatry. 2021 Dec 24;12:800047. doi: 10.3389/fpsyt.2021.800047. eCollection 2021. Front Psychiatry. 2021. PMID: 35002814 Free PMC article.
-
Obsessive-compulsive symptoms and traits in patients with burning mouth syndrome: a cross-sectional multicentric analysis.Clin Oral Investig. 2025 Apr 5;29(4):223. doi: 10.1007/s00784-025-06293-6. Clin Oral Investig. 2025. PMID: 40186752 Free PMC article.
References
-
- American Psychiatric Association; (2000). Diagnostic and Statistical Manual of Mental Disorders (DSM–V–TR) 4th ed Washington, DC.
-
- American Psychiatric Association; (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed; American Psychiatric Publishing: Washington, DC: Retrieved from http://psychiatryonline.org.libdata.lib.ua.edu/
-
- American Academy of Sleep Medicine. (2005). International classification of sleep disorders: Diagnostic and coding manual, 2nd Ed Westchester: American Academy of Sleep Medicine.
-
- Bonnet MH, & Arand DL (2010). Hyperarousal and insomnia: State of the science. Sleep Medicine Reviews, 14, 9–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical