

Therapeutic approaches for cardiac regeneration and repair
- PMID: 29872165
- PMCID: PMC6241533
- DOI: 10.1038/s41569-018-0036-6
Therapeutic approaches for cardiac regeneration and repair
Abstract
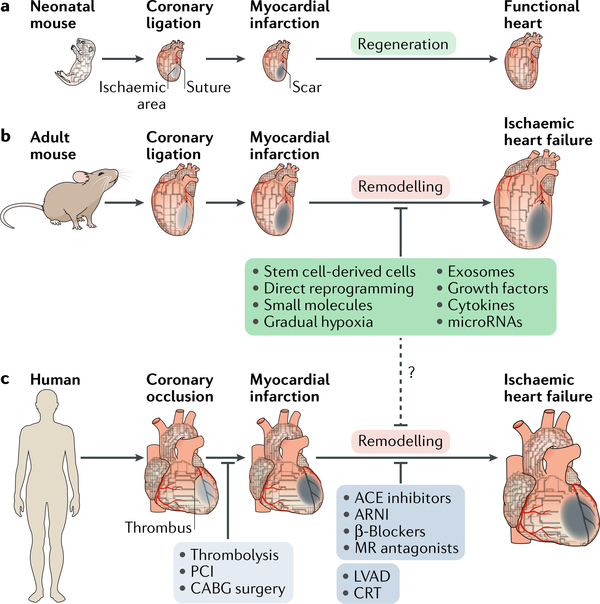
Ischaemic heart disease is a leading cause of death worldwide. Injury to the heart is followed by loss of the damaged cardiomyocytes, which are replaced with fibrotic scar tissue. Depletion of cardiomyocytes results in decreased cardiac contraction, which leads to pathological cardiac dilatation, additional cardiomyocyte loss, and mechanical dysfunction, culminating in heart failure. This sequential reaction is defined as cardiac remodelling. Many therapies have focused on preventing the progressive process of cardiac remodelling to heart failure. However, after patients have developed end-stage heart failure, intervention is limited to heart transplantation. One of the main reasons for the dramatic injurious effect of cardiomyocyte loss is that the adult human heart has minimal regenerative capacity. In the past 2 decades, several strategies to repair the injured heart and improve heart function have been pursued, including cellular and noncellular therapies. In this Review, we discuss current therapeutic approaches for cardiac repair and regeneration, describing outcomes, limitations, and future prospects of preclinical and clinical trials of heart regeneration. Substantial progress has been made towards understanding the cellular and molecular mechanisms regulating heart regeneration, offering the potential to control cardiac remodelling and redirect the adult heart to a regenerative state.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures

References
-
- Cohn JN, Ferrari R & Sharpe N Cardiac remodeling — concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. J. Am. Coll. Cardiol. 35, 569–582 (2000). - PubMed
-
- Sacks CA, Jarcho JA & Curfman GD Paradigm shifts in heart-failure therapy — a timeline. N. Engl. J. Med. 371,989–991 (2014). - PubMed
-
- Packer M et al. Effect of carvedilol on survival in severe chronic heart failure. N. Engl. J. Med. 344, 1651–1658 (2001). - PubMed
-
- The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N. Engl. J. Med. 325, 293–302 (1991). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
