

Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration
- PMID: 29872859
- PMCID: PMC6583054
- DOI: 10.1001/jama.2018.5725
Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration
Erratum in
-
Data Errors in Figure 3 and Labels Transposed in Figure 4.JAMA. 2018 Jul 17;320(3):308. doi: 10.1001/jama.2018.9635. JAMA. 2018. PMID: 30027228 Free PMC article. No abstract available.
Abstract
Importance: There are potential benefits and harms of hyperoxemia and hypoxemia for extremely preterm infants receiving more vs less supplemental oxygen.
Objective: To compare the effects of different target ranges for oxygen saturation as measured by pulse oximetry (Spo2) on death or major morbidity.
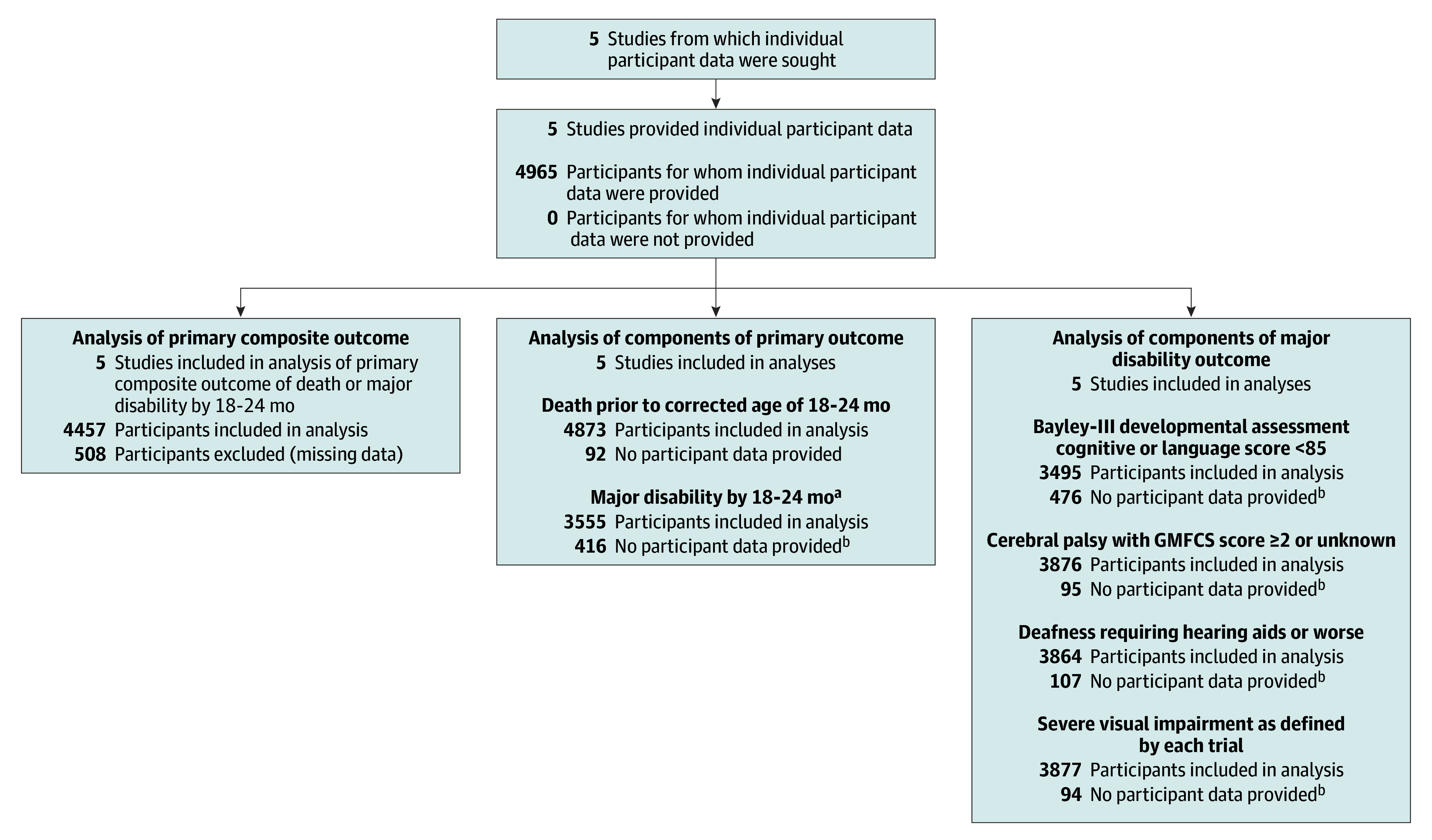
Design, setting, and participants: Prospectively planned meta-analysis of individual participant data from 5 randomized clinical trials (conducted from 2005-2014) enrolling infants born before 28 weeks' gestation.
Exposures: Spo2 target range that was lower (85%-89%) vs higher (91%-95%).
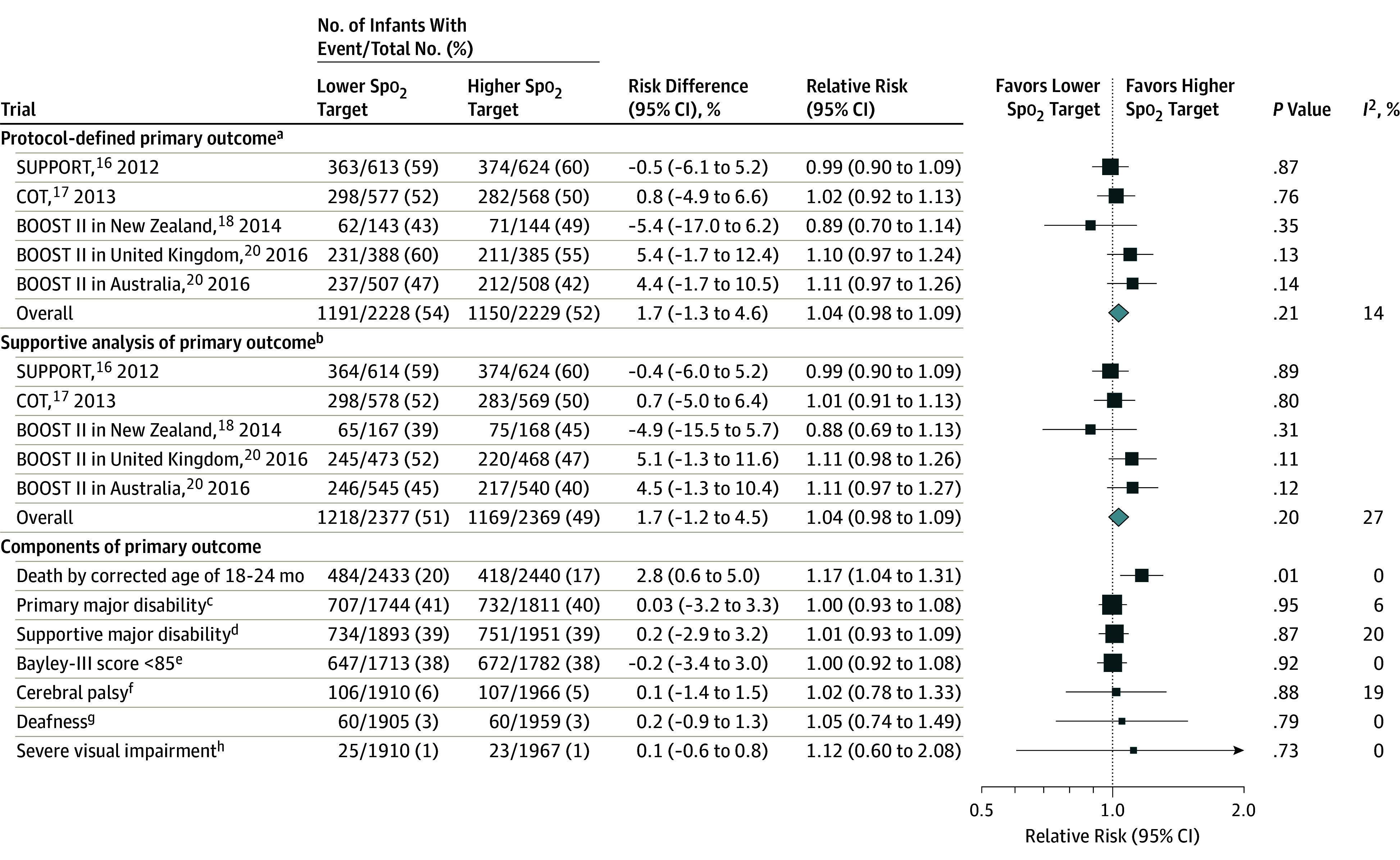
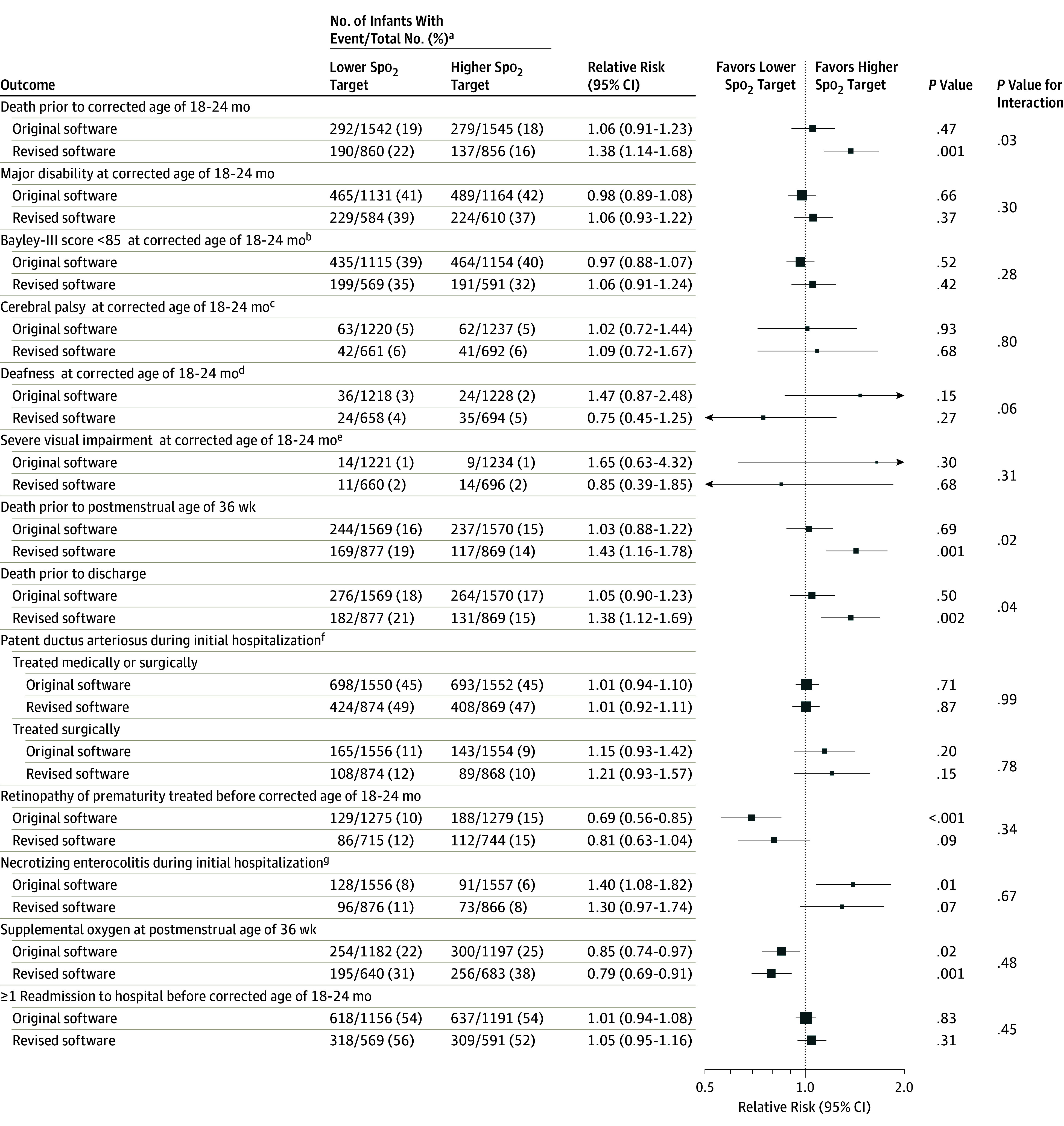
Main outcomes and measures: The primary outcome was a composite of death or major disability (bilateral blindness, deafness, cerebral palsy diagnosed as ≥2 level on the Gross Motor Function Classification System, or Bayley-III cognitive or language score <85) at a corrected age of 18 to 24 months. There were 16 secondary outcomes including the components of the primary outcome and other major morbidities.
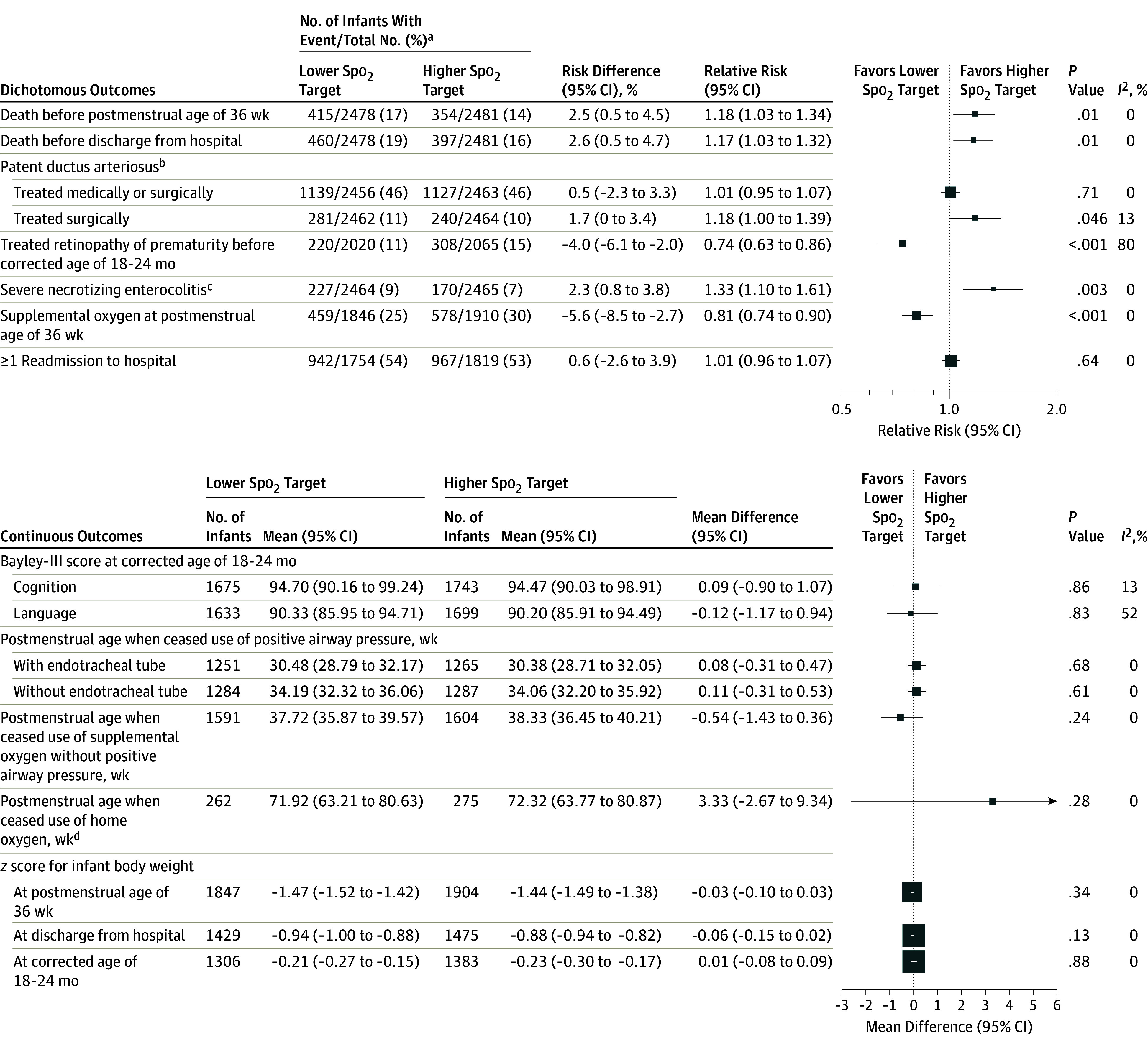
Results: A total of 4965 infants were randomized (2480 to the lower Spo2 target range and 2485 to the higher Spo2 range) and had a median gestational age of 26 weeks (interquartile range, 25-27 weeks) and a mean birth weight of 832 g (SD, 190 g). The primary outcome occurred in 1191 of 2228 infants (53.5%) in the lower Spo2 target group and 1150 of 2229 infants (51.6%) in the higher Spo2 target group (risk difference, 1.7% [95% CI, -1.3% to 4.6%]; relative risk [RR], 1.04 [95% CI, 0.98 to 1.09], P = .21). Of the 16 secondary outcomes, 11 were null, 2 significantly favored the lower Spo2 target group, and 3 significantly favored the higher Spo2 target group. Death occurred in 484 of 2433 infants (19.9%) in the lower Spo2 target group and 418 of 2440 infants (17.1%) in the higher Spo2 target group (risk difference, 2.8% [95% CI, 0.6% to 5.0%]; RR, 1.17 [95% CI, 1.04 to 1.31], P = .01). Treatment for retinopathy of prematurity was administered to 220 of 2020 infants (10.9%) in the lower Spo2 target group and 308 of 2065 infants (14.9%) in the higher Spo2 target group (risk difference, -4.0% [95% CI, -6.1% to -2.0%]; RR, 0.74 [95% CI, 0.63 to 0.86], P < .001). Severe necrotizing enterocolitis occurred in 227 of 2464 infants (9.2%) in the lower Spo2 target group and 170 of 2465 infants (6.9%) in the higher Spo2 target group (risk difference, 2.3% [95% CI, 0.8% to 3.8%]; RR, 1.33 [95% CI, 1.10 to 1.61], P = .003).
Conclusions and relevance: In this prospectively planned meta-analysis of individual participant data from extremely preterm infants, there was no significant difference between a lower Spo2 target range compared with a higher Spo2 target range on the primary composite outcome of death or major disability at a corrected age of 18 to 24 months. The lower Spo2 target range was associated with a higher risk of death and necrotizing enterocolitis, but a lower risk of retinopathy of prematurity treatment.
Conflict of interest statement
Figures
Comment in
-
Optimizing Oxygen Saturation Targets in Extremely Preterm Infants.JAMA. 2018 Jun 5;319(21):2173-2174. doi: 10.1001/jama.2018.5724. JAMA. 2018. PMID: 29872840 No abstract available.
-
Should we target higher or lower oxygen saturation targets in the preterm infant?J Perinatol. 2019 May;39(5):758-760. doi: 10.1038/s41372-019-0325-x. Epub 2019 Jan 28. J Perinatol. 2019. PMID: 30692618 No abstract available.
References
-
- Askie LM, Henderson-Smart DJ. Restricted versus liberal oxygen exposure for preventing morbidity and mortality in preterm or low birth weight infants. Cochrane Database Syst Rev. 2001;4(4):CD001077. - PubMed
-
- STOP-ROP Investigators . Supplemental therapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP), a randomized, controlled trial, I: primary outcomes. Pediatrics. 2000;105(2):295-310. - PubMed
-
- Askie LM, Henderson-Smart DJ, Irwig L, Simpson JM. Oxygen-saturation targets and outcomes in extremely preterm infants. N Engl J Med. 2003;349(10):959-967. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R03 HD079867/HD/NICHD NIH HHS/United States
- M01 RR000044/RR/NCRR NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- M01 RR006022/RR/NCRR NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- M01 RR007122/RR/NCRR NIH HHS/United States
- UL1 RR025744/RR/NCRR NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD053124/HD/NICHD NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- CIHR/Canada
- U10 HD021397/HD/NICHD NIH HHS/United States
- M01 RR000054/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- M01 RR016587/RR/NCRR NIH HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U10 HD053119/HD/NICHD NIH HHS/United States
- UL1 RR024979/RR/NCRR NIH HHS/United States
- M01 RR000633/RR/NCRR NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- M01 RR000059/RR/NCRR NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- M01 RR000030/RR/NCRR NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
- M01 RR000032/RR/NCRR NIH HHS/United States
- G0400415/MRC_/Medical Research Council/United Kingdom
- M01 RR000997/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- M01 RR000064/RR/NCRR NIH HHS/United States
