

The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients
- PMID: 29872882
- PMCID: PMC6013508
- DOI: 10.1007/s00134-018-5218-5
The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients
Abstract
Purpose: Current guidelines recommend maintaining a mean arterial pressure (MAP) ≥ 65 mmHg in septic patients. However, the relationship between hypotension and major complications in septic patients remains unclear. We, therefore, evaluated associations of MAPs below various thresholds and in-hospital mortality, acute kidney injury (AKI), and myocardial injury.
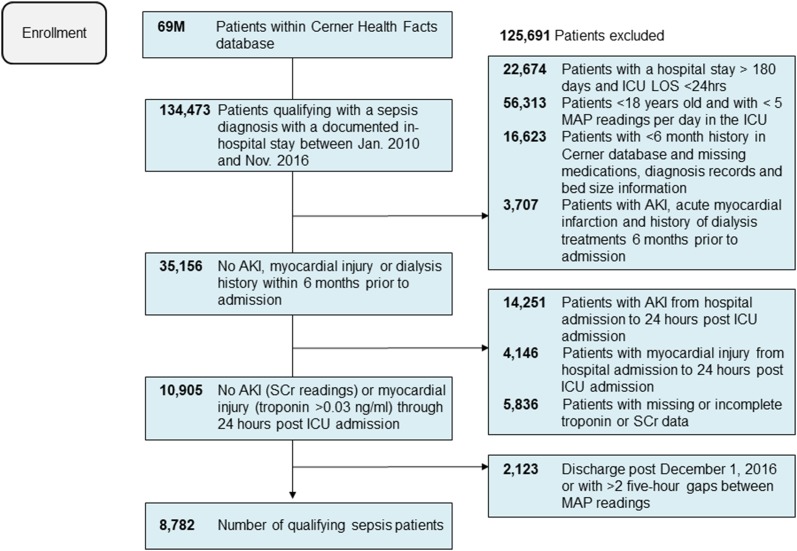
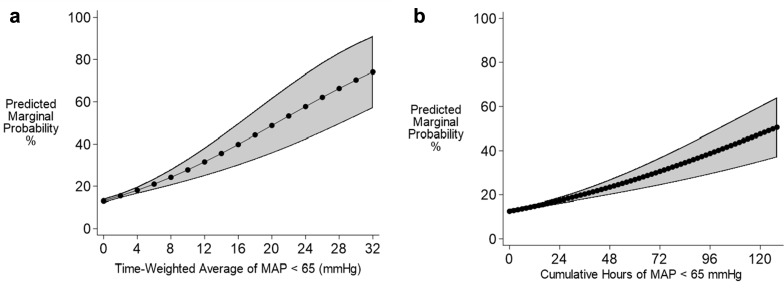
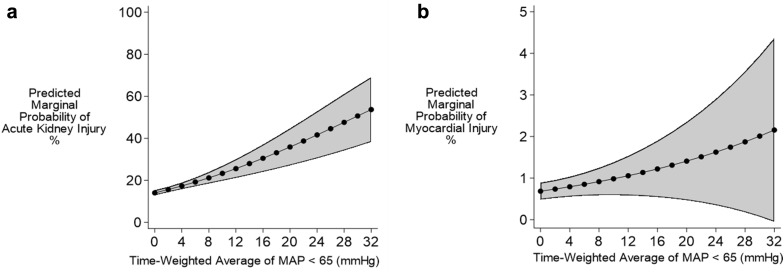
Methods: We conducted a retrospective analysis using electronic health records from 110 US hospitals. We evaluated septic adults with intensive care unit (ICU) stays ≥ 24 h from 2010 to 2016. Patients were excluded with inadequate blood pressure recordings, poorly documented potential confounding factors, or renal or myocardial histories documented within 6 months of ICU admission. Hypotension exposure was defined by time-weighted average mean arterial pressure (TWA-MAP) and cumulative time below 55, 65, 75, and 85 mmHg thresholds. Multivariable logistic regressions determined the associations between hypotension exposure and in-hospital mortality, AKI, and myocardial injury.
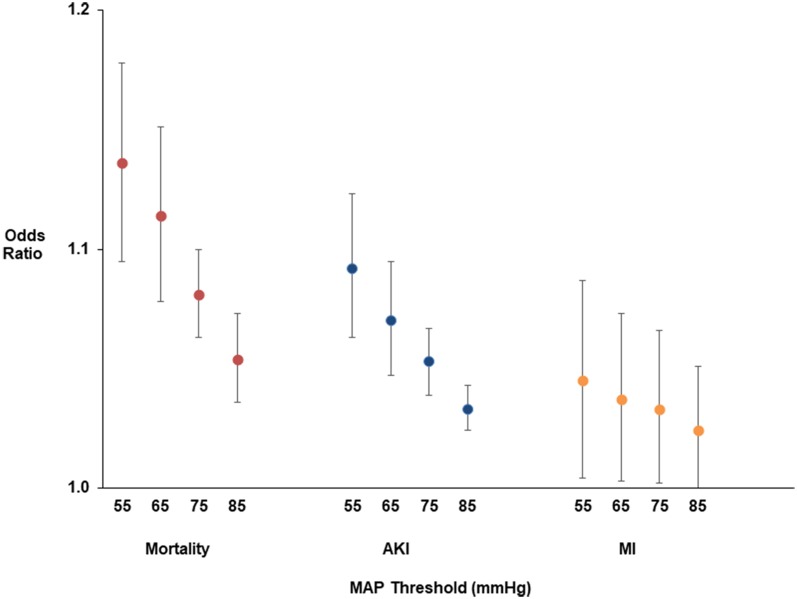
Results: In total, 8,782 patients met study criteria. For every one unit increase in TWA-MAP < 65 mmHg, the odds of in-hospital mortality increased 11.4% (95% CI 7.8%, 15.1%, p < 0.001); the odds of AKI increased 7.0% (4.7, 9.5%, p < 0.001); and the odds of myocardial injury increased 4.5% (0.4, 8.7%, p = 0.03). For mortality and AKI, odds progressively increased as thresholds decreased from 85 to 55 mmHg.
Conclusions: Risks for mortality, AKI, and myocardial injury were apparent at 85 mmHg, and for mortality and AKI risk progressively worsened at lower thresholds. Maintaining MAP well above 65 mmHg may be prudent in septic ICU patients.
Keywords: Acute kidney injury; Blood pressure monitoring; Hypotension; Mortality; Myocardial injury; Sepsis.
Conflict of interest statement
Drs. Maheshwari and Sessler work as consultants for Edwards Lifesciences. Dr. Khanna consults for La Jolla pharmaceuticals. Drs. Khangulov, Munson and Badani work as consultants for Boston Strategic Partners, Inc. who received funds from Edwards Lifesciences to perform the research. Dr. Nathanson is an employee of OptiStatim, LLC, which received consulting fees from Boston Strategic Partners, Inc.
Figures
Comment in
-
MAP of 65: target of the past?Intensive Care Med. 2018 Sep;44(9):1551-1552. doi: 10.1007/s00134-018-5292-8. Epub 2018 Jul 12. Intensive Care Med. 2018. PMID: 30003302 No abstract available.
-
Should we treat mild hypotension in septic patients in the absence of peripheral tissue hypoperfusion?Intensive Care Med. 2018 Sep;44(9):1593-1594. doi: 10.1007/s00134-018-5315-5. Epub 2018 Jul 21. Intensive Care Med. 2018. PMID: 30032430 No abstract available.
References
-
- Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011;62:1–8. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45:486–552. doi: 10.1097/CCM.0000000000002255. - DOI - PubMed
-
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM, Shankar-Hari M, Singer M, Deutschman CS, Escobar GJ, Angus DC. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315:762–774. doi: 10.1001/jama.2016.0288. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
