

Follow-up of parenchymal changes in the thyroid gland with diffuse autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma
- PMID: 29872995
- PMCID: PMC6394764
- DOI: 10.1007/s40618-018-0909-x
Follow-up of parenchymal changes in the thyroid gland with diffuse autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma
Abstract
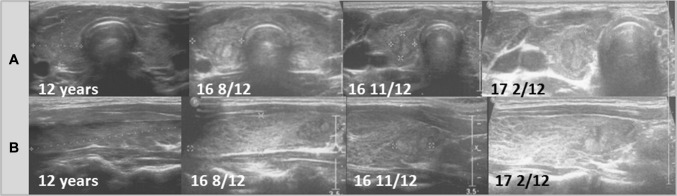
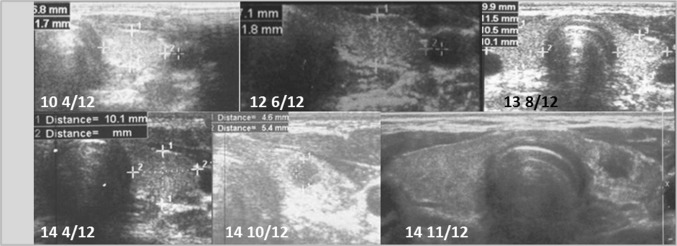
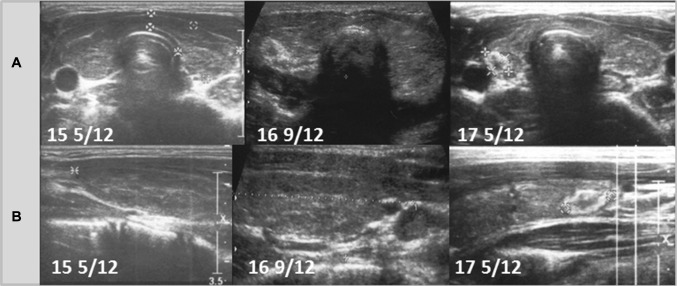
Purpose: To present the outcomes of ultrasound (US) follow-ups in children with autoimmune thyroid disease who did not have a thyroid nodule on admission but developed papillary thyroid carcinoma (PTC) and to characterize the parenchymal changes in the thyroid gland prior to the development of PTC.
Methods: A retrospective thyroid US scan review of 327 patients diagnosed with AIT was performed. Forty patients (40/327, 12.2%) presented nodular AIT variant with a normoechogenic background. Eleven patients (11/327, 3.4%, 11/40, 27.5%) presenting this variant were diagnosed with PTC (nine females-mean age 15.3 years; two males aged 11 and 13 years). In five of 11 patients, the suspicious nodule that was later confirmed to be PTC was detected on the initial US at presentation. For the remaining six females (6/11) who developed PTC during the follow-up, we retrospectively analysed their US thyroid scans and these patients were selected for analysis in this study.
Results: On admission, the US evaluation revealed an enlarged normoechogenic thyroid gland in three patients and a hypoechogenic thyroid gland with fibrosis as indicated by irregular, chaotic hyperechogenic layers in three patients. No thyroid nodules were identified. Ultrasound monitoring revealed increasing echogenicity of the thyroid parenchyma during the follow-up. PTC developed in a mean time of 4.6 years (1 9/12-7 4/12 years) since referral to the outpatient thyroid clinic and 2.9 years (6/12-6 9/12) since the last nodule-free US thyroid scan.
Conclusions: Sonographic follow-up assessments warrant further exploration as a strategy to determine PTC susceptibility in the paediatric population.
Keywords: Autoimmune thyroiditis; Normoechogenic background of thyroid gland; Papillary thyroid carcinoma; Ultrasonography of thyroid gland.
Conflict of interest statement
Conflict of interests
The authors have nothing to disclose and there are no conflicts of interests.
Ethical approval
The authors confirm that this retrospective work was performed in compliance with Ethical Standards and according to Institutional Review Board standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures



References
-
- Koney N, Mahmood S, Gannon A, Finkelstein MS, Mody T. Pediatric thyroid cancer: imaging and therapy update. Curr Radiol Rep. 2017;5:48. doi: 10.1007/s40134-017-0247-3. - DOI
-
- Niedziela M, Handkiewicz-Junak D, Małecka-Tendera E, Czarniecka A, Dedecjus M, Lange D, Kucharska A, Gawlik A, Pomorski L, Włoch J, et al. Diagnostics and treatment of differentiated thyroid carcinoma in children—guidelines of polish national societies. Endokrynol Pol. 2016;67:628–642. doi: 10.5603/EP.2016.0072. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
