

Prevalence and features of asthma-COPD overlap in the United States 2007-2012
- PMID: 29873189
- PMCID: PMC6287748
- DOI: 10.1111/crj.12917
Prevalence and features of asthma-COPD overlap in the United States 2007-2012
Abstract
Background: Perceived to be distinct, asthma and chronic obstructive pulmonary disease (COPD) can co-exist and potentially have a worse prognosis than the separate diseases. Yet, little is known about the exact prevalence and the characteristics of the Asthma-COPD overlap (ACO) in the US population.
Aims: To determine ACO prevalence in the United States, identify ACO predictors, examine ACO association with asthma and COPD severity, and describe distinctive spirometry and laboratory features of ACO.
Methods: Data on adult participants to the National Health and Nutrition Examination Surveys conducted from 2007 to 2012 was analyzed. ACO was defined as current asthma and post-bronchodilator forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) <0.7.
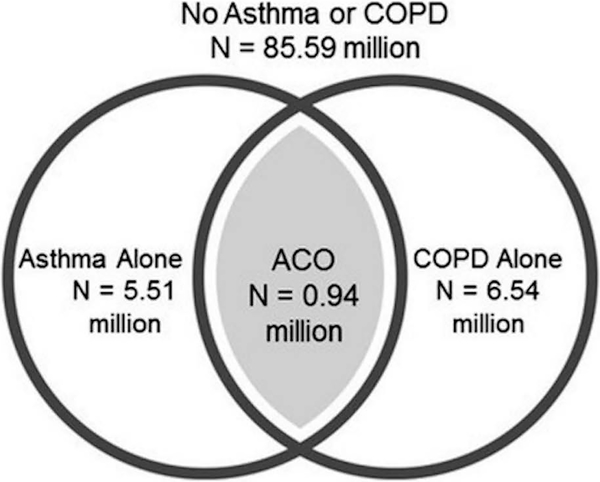
Results: Overall, 7,570 participants representing 98.58 million Americans were included in our study. From 2007 to 2012, the crude and age-standardized ACO prevalence were, respectively, 0.96% (95% CI: 0.65%-1.26%) and 1.05% (0.74%-1.37%). In asthma, ACO predictors included older age, male gender, and smoking. In COPD, ACO predictors were non-Hispanic Black race/ethnicity and obesity. ACO was associated with increased ER visits for asthma (OR = 3.46, 95% CI: 1.48-8.06]) and oxygen therapy in COPD (OR = 11.17, 95% CI: 5.17-24.12]). In spirometry, FEV1 and peak expiratory flow were lower in ACO than in asthma or COPD alone.
Conclusion: Age-adjusted prevalence of ACO in the United States was 1.05% in 2007-2012, representing 0.94 (95% CI: 0.62-1.26) million Americans. It is much lower than previously reported. The overlap was associated with higher asthma and COPD severity as well as decreased lung function compared with COPD or asthma alone.
Keywords: ACO; ACOS; COPD; asthma; asthma-COPD overlap; prevalence.
© 2018 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Yamauchi Y, Yasunaga H, Matsui H, Hasegawa W, Jo T, Takami K, et al. Comparison of in‐hospital mortality in patients with COPD, asthma and asthma–COPD overlap exacerbations. Respirology. 2015;20(6):940–6. - PubMed
-
- Lambrecht B, Hammad H. Asthma and coagulation. N Engl J Med. 2013;369(20):1964–6. - PubMed
-
- Barnes PJ. Mechanisms in COPD: differences from asthma. Chest. 2000;117(2_suppl):10S–4S. - PubMed
-
- Barnes PJ. Mechanisms and resistance in glucocorticoid control of inflammation. J Steroid Biochem Mol Biol. 2010;120(2):76–85. - PubMed
-
- Postma DS, Rabe KF. The asthma–COPD overlap syndrome. N Engl J Med. 2015;373(13):1241–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
