

Fluid balance-adjusted creatinine at initiation of continuous venovenous hemofiltration and mortality. A post-hoc analysis of a multicenter randomized controlled trial
- PMID: 29874271
- PMCID: PMC5991340
- DOI: 10.1371/journal.pone.0197301
Fluid balance-adjusted creatinine at initiation of continuous venovenous hemofiltration and mortality. A post-hoc analysis of a multicenter randomized controlled trial
Abstract
Introduction: Acute kidney injury (AKI) requiring renal replacement therapy (RRT) is associated with high mortality. The creatinine-based stage of AKI is considered when deciding to start or delay RRT. However, creatinine is not only determined by renal function (excretion), but also by dilution (fluid balance) and creatinine generation (muscle mass). The aim of this study was to explore whether fluid balance-adjusted creatinine at initiation of RRT is related to 28-day mortality independent of other markers of AKI, surrogates of muscle mass and severity of disease.
Methods: We performed a post-hoc analysis on data from the multicentre CASH trial comparing citrate to heparin anticoagulation during continuous venovenous hemofiltration (CVVH). To determine whether fluid balance-adjusted creatinine was associated with 28-day mortality, we performed a logistic regression analysis adjusting for confounders of creatinine generation (age, gender, body weight), other markers of AKI (creatinine, urine output) and severity of disease.
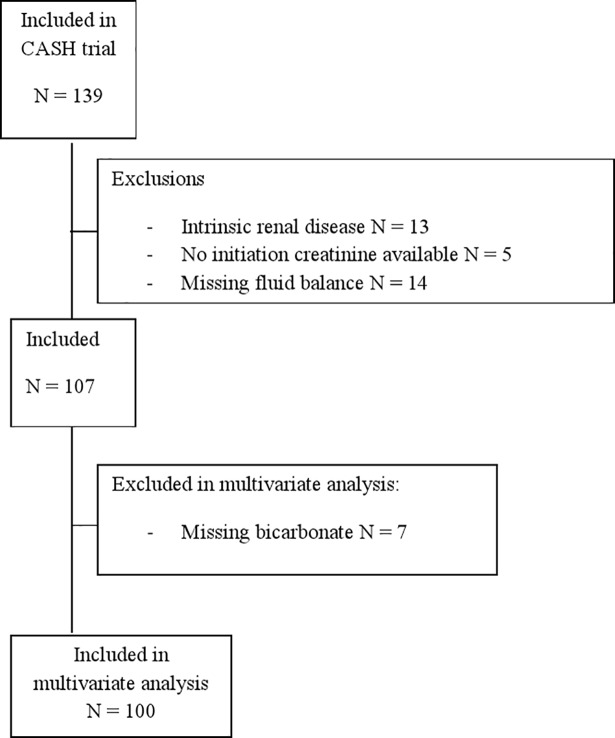
Results: Of the 139 patients, 32 patients were excluded. Of the 107 included patients, 36 died at 28 days (34%). Non-survivors were older, had higher APACHE II and inclusion SOFA scores, lower pH and bicarbonate, lower creatinine and fluid balance-adjusted creatinine at CVVH initiation. In multivariate analysis lower fluid balance-adjusted creatinine (OR 0.996, 95% CI 0.993-0.999, p = 0.019), but not unadjusted creatinine, remained associated with 28-day mortality together with bicarbonate (OR 0.869, 95% CI 0.769-0.982, P = 0.024), while the APACHE II score non-significantly contributed to the model.
Conclusion: In this post-hoc analysis of a multicentre trial, low fluid balance-adjusted creatinine at CVVH initiation was associated with 28-day mortality, independent of other markers of AKI, organ failure, and surrogates of muscle mass, while unadjusted creatinine was not. More tools are needed for better understanding of the complex determinants of "AKI classification", "CVVH initiation" and their relation with mortality, fluid balance is only one.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: HOvS has received research support from Dirinco, and honoraria and speaker's fees from Gambro/Baxter and Fresenius in the past. SN received honoraria/grants from Astellas, Chiesi and Novartis. MV received honoraria from Astellas, Amgen and Baxter in the past and is currently receiving research grants from Shire, Sanofi and Fresenius. This does not alter our adherence to PLOS ONE policies on sharing data and materials. The remaining authors declare that they have no competing interests.
Figures

References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–8. doi: 10.1001/jama.294.7.813 - DOI - PubMed
-
- Kellum JA, Lameire N, Group KAGW. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Critical care. 2013;17(1):204 doi: 10.1186/cc11454 - DOI - PMC - PubMed
-
- Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Critical care. 2007;11(2):R31 doi: 10.1186/cc5713 - DOI - PMC - PubMed
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative w. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Critical care. 2004;8(4):R204–12. doi: 10.1186/cc2872 - DOI - PMC - PubMed
-
- Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nature reviews Nephrology. 2017;13(4):241–57. doi: 10.1038/nrneph.2017.2 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
