

Repeated in-field radiosurgery for locally recurrent brain metastases: Feasibility, results and survival in a heavily treated patient cohort
- PMID: 29874299
- PMCID: PMC5991396
- DOI: 10.1371/journal.pone.0198692
Repeated in-field radiosurgery for locally recurrent brain metastases: Feasibility, results and survival in a heavily treated patient cohort
Abstract
Purpose: Stereotactic radiosurgery (SRS) is an established primary treatment for newly diagnosed brain metastases with high local control rates. However, data about local re-irradiation in case of local failure after SRS (re-SRS) are rare. We evaluated the feasibility, efficacy and patient selection characteristics in treating locally recurrent metastases with a second course of SRS.
Methods: We retrospectively evaluated patients with brain metastases treated with re-SRS for local tumor progression between 2011 and 2017. Patient and treatment characteristics as well as rates of tumor control, survival and toxicity were analyzed.
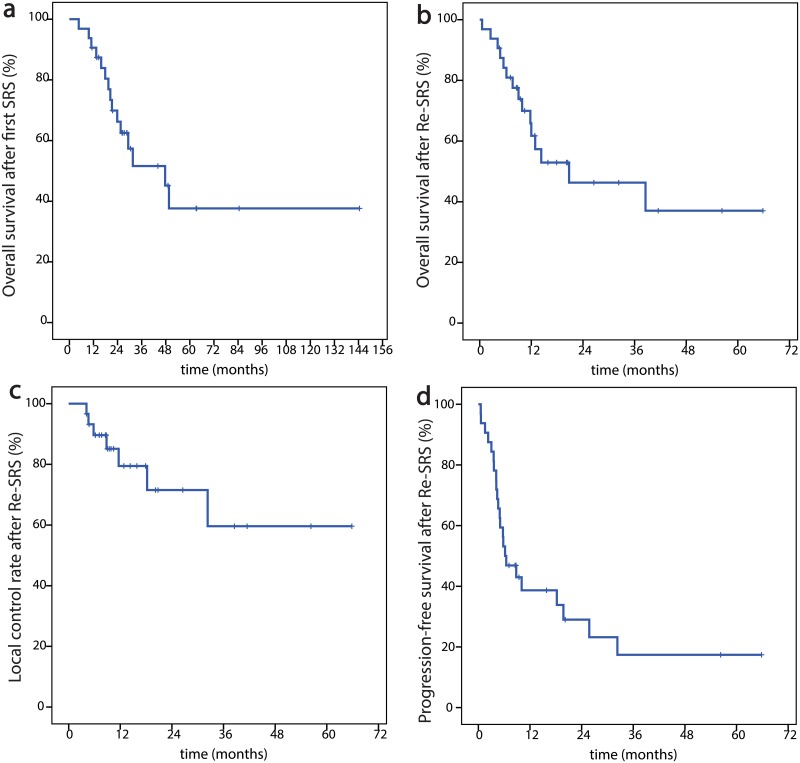
Results: Overall, 32 locally recurrent brain metastases in 31 patients were irradiated with re-SRS. Median age at re-SRS was 64.9 years. The primary histology was breast cancer and non-small-cellular lung cancer (NSCLC) in respectively 10 cases (31.3%), in 5 cases malignant melanoma (15.6%). In the first SRS-course 19 metastases (59.4%) and in the re-SRS-course 29 metastases (90.6%) were treated with CyberKnife® and the others with Gamma Knife. Median planning target volume (PTV) for re-SRS was 2.5 cm3 (range, 0.1-37.5 cm3) and median dose prescribed to the PTV was 19 Gy (range, 12-28 Gy) in 1-5 fractions to the median 69% isodose (range, 53-80%). The 1-year overall survival rate was 61.7% and the 1-year local control rate was 79.5%. The overall rate of radiological radio-necrosis was 16.1% and four patients (12.9%) experienced grade ≥ 3 toxicities.
Conclusions: A second course of SRS for locally recurrent brain metastases after prior local SRS appears to be feasible with acceptable toxicity and can be considered as salvage treatment option for selected patients with high performance status. Furthermore, this is the first study utilizing robotic radiosurgery for this indication, as an additional option for frameless fractionated treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Linskey ME, Andrews DW, Asher AL, Burri SH, Kondziolka D, Robinson PD, et al. The role of stereotactic radiosurgery in the management of patients with newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline. Journal of Neuro-Oncology. 2010;96(1):45–68. doi: 10.1007/s11060-009-0073-4 - DOI - PMC - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA. 2006;295(21):2483–91. doi: 10.1001/jama.295.21.2483 - DOI - PubMed
-
- Kocher M, Soffietti R, Abacioglu U, Villà S, Fauchon F, Baumert BG, et al. Adjuvant Whole-Brain Radiotherapy Versus Observation After Radiosurgery or Surgical Resection of One to Three Cerebral Metastases: Results of the EORTC 22952–26001 Study. Journal of Clinical Oncology. 2011;29(2):134–41. doi: 10.1200/JCO.2010.30.1655 - DOI - PMC - PubMed
-
- Brown PD, Ballman KV, Cerhan JH, Anderson SK, Carrero XW, Whitton AC, et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): a multicentre, randomised, controlled, phase 3 trial. The Lancet Oncology. 2017;18(8):1049–60. doi: 10.1016/S1470-2045(17)30441-2 - DOI - PMC - PubMed
-
- Mahajan A, Ahmed S, McAleer MF, Weinberg JS, Li J, Brown P, et al. Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: a single-centre, randomised, controlled, phase 3 trial. The Lancet Oncology. 2017;18(8):1040–8. doi: 10.1016/S1470-2045(17)30414-X - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
