

Association of Plane of Total Mesorectal Excision With Prognosis of Rectal Cancer: Secondary Analysis of the CAO/ARO/AIO-04 Phase 3 Randomized Clinical Trial
- PMID: 29874375
- PMCID: PMC6142959
- DOI: 10.1001/jamasurg.2018.1607
Association of Plane of Total Mesorectal Excision With Prognosis of Rectal Cancer: Secondary Analysis of the CAO/ARO/AIO-04 Phase 3 Randomized Clinical Trial
Abstract
Importance: Previous retrospective studies have shown that surgical quality affects local control in rectal cancer..
Objective: In this secondary end point analysis, we evaluated the prognostic effect of the total mesorectal excision (TME) plane in the CAO/ARO/AIO-04 phase 3 randomized clinical trial.
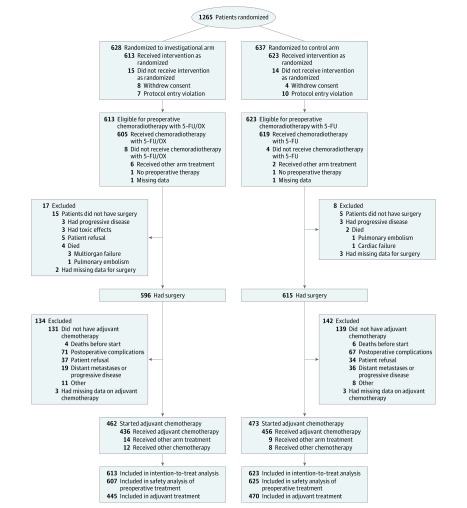
Design, setting, and participants: The CAO/ARO/AIO-04 trial enrolled 1236 patients with cT3-4 and/or node-positive rectal adenocarcinoma from 88 centers in Germany between July 25, 2006, and February 26, 2010.
Interventions: Patients were randomized to receive treatment with standard fluorouracil-based preoperative chemoradiotherapy (CRT) alone (control arm) or oxaliplatin (experimental arm) followed by TME and adjuvant chemotherapy.
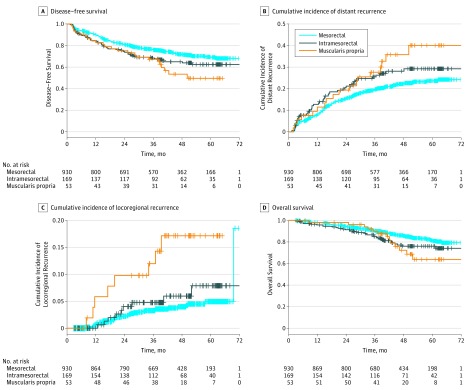
Main outcomes and measures: The TME quality (mesorectal, intramesorectal, and muscularis propria plane) was prospectively assessed in 1152 operation specimens. An assessment was performed independently by pathologists and surgeons. The results were correlated with clinicopathologic data and the clinical outcome was tested, including multivariable analysis with the Cox regression model.
Results: Of 1152 German Caucasian participants, 332 (28.8) were women and the mean age was 63 years. The plane of TME was mesorectal in 930 patients (80.7%), intramesorectal in 169 (14.7%), and muscularis propria in 53 (4.6%). In a univariable analysis, the TME plane was significantly associated with 3-year disease-free survival (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 73.1-78.8 vs 61.6-76.0 vs 55.6-81.3, respectively; P = .01), cumulative incidence of local and distant recurrences (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 2.0-4.5 vs 1.2-8.1 vs 2.5-20.5, respectively; P < .001; and mesorectal vs intramesorectal vs muscularis propria, 95% CI, 17.0-22.4 vs 18.3-32.0 vs 14.2-39.0, respectively; P = .03, respectively), and overall survival (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 88.3-92.3 vs 79.7-91.0 vs 81.6-98.7, respectively; P = .02). In contrast to the pathologist-based evaluation, the assessment of TME plane by the operating surgeon failed to demonstrate prognostic significance for any of these clinical end points. In a multivariable analysis, the plane of surgery (mesorectal vs muscularis propria TME) constituted an independent factor for local recurrence (P = .002).
Conclusions and relevance: This phase 3 randomized clinical trial confirms the long-term clinical effect of TME plane quality on local recurrence, as initially reported in the MRC CR07 study. The data highlight the key role of pathologists and surgeons in the multidisciplinary management of rectal cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT00349076.
Conflict of interest statement
Figures
Comment in
-
Locally Advanced Rectal Cancer: Is It Time for a Paradigm Change?JAMA Surg. 2018 Aug 1;153(8):e181620. doi: 10.1001/jamasurg.2018.1620. Epub 2018 Aug 15. JAMA Surg. 2018. PMID: 29874379 No abstract available.
-
Interpreting the Long-term Prognostic Value of Total Mesorectal Excision Plane Quality in Rectal Adenocarcinoma.JAMA Surg. 2019 Jan 1;154(1):96. doi: 10.1001/jamasurg.2018.3540. JAMA Surg. 2019. PMID: 30427976 No abstract available.
References
-
- Sauer R, Becker H, Hohenberger W, et al. ; German Rectal Cancer Study Group . Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):-. - PubMed
-
- Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. ; Dutch Colorectal Cancer Group . Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345(9):638-646. - PubMed
-
- Folkesson J, Birgisson H, Pahlman L, Cedermark B, Glimelius B, Gunnarsson U. Swedish Rectal Cancer Trial: long lasting benefits from radiotherapy on survival and local recurrence rate. J Clin Oncol. 2005;23(24):5644-5650. - PubMed
-
- Quirke P. Training and quality assurance for rectal cancer: 20 years of data is enough. Lancet Oncol. 2003;4(11):695-702. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
