

Comparative addition of dexmedetomidine and fentanyl to intrathecal bupivacaine in orthopedic procedure in lower limbs
- PMID: 29875020
- PMCID: PMC5991430
- DOI: 10.1186/s12871-018-0531-7
Comparative addition of dexmedetomidine and fentanyl to intrathecal bupivacaine in orthopedic procedure in lower limbs
Abstract
Background: Spinal block is a common procedure for lower limbs surgery. Fentanyl, a synthetic opioid and dexmedetomidine, a selective α2 agonist have been used as adjuvants in spinal anesthesia to prolong intraoperative and postoperative analgesia. The aim of current study is to compare the efficacy of dexmedetomidine and fentanyl added to intrathecal bupivacaine in orthopedic procedures in lower limbs.
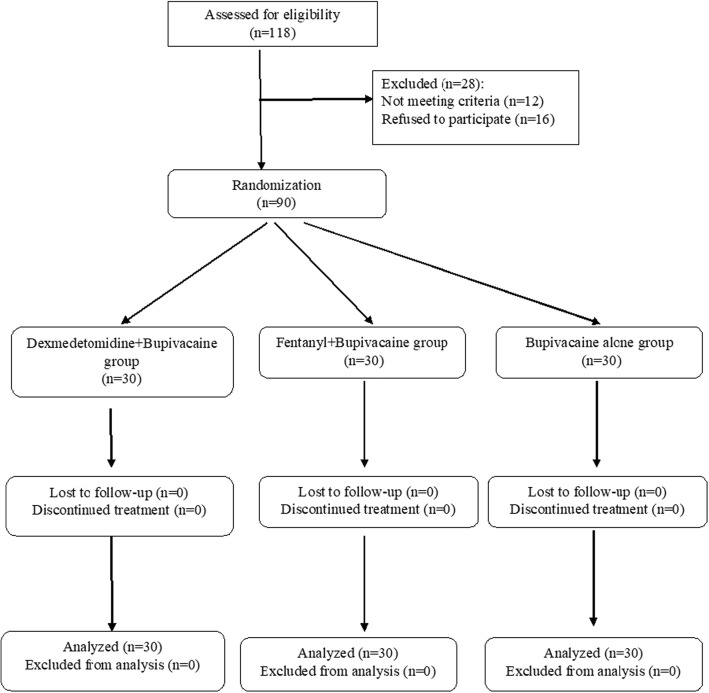
Methods: In this randomized clinical trial, 90 patients undergoing elective lower limb surgeries were randomly allocated to three groups. Via intrathecal approach, the patients received 2.5 ml hyperbaric bupivacaine 0.5% plus 5 micrograms dexmedetomidine (BD group), 25 micrograms fentanyl (BF group) or 0.5 ml normal saline (BN group), respectively. Time to reach the complete motor block, the highest sensory level, regression from block, analgesic request and duration of the drug effect, hemodynamic changes and side effects were compared between the groups.
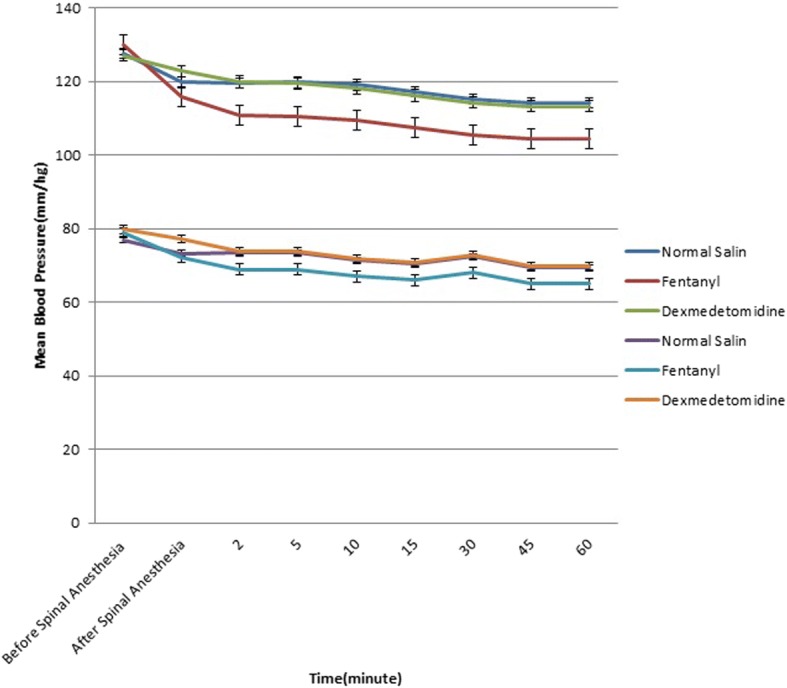
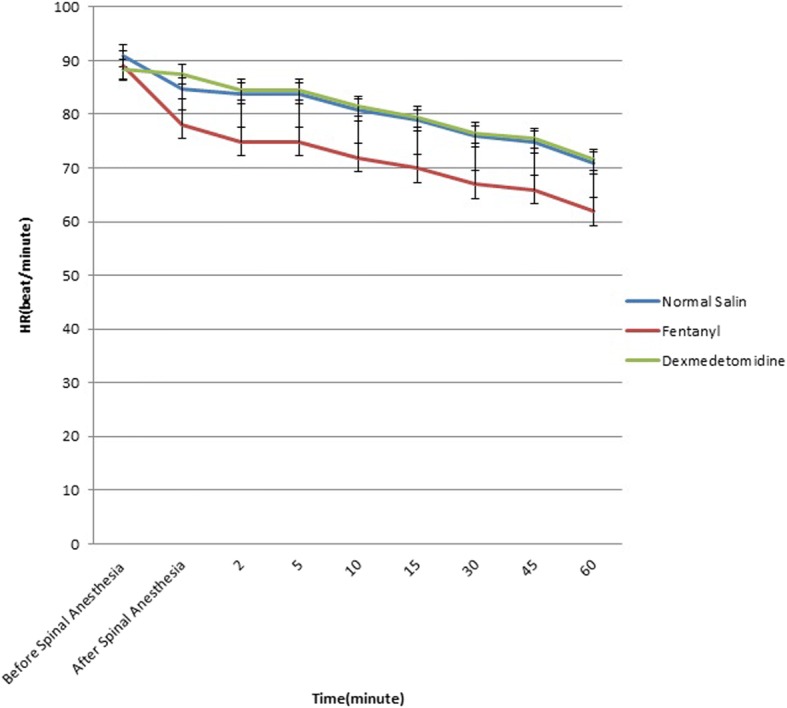
Results: There was no significant difference between the groups regrading time to reach complete motor block, but time to reach the highest sensory level was shorter in group BD than group BF (6.28 ± 1.75 vs. 7.17 ± 1.45, p = 0.03). Group BD had significantly lower mean of NRS 6 h after operation (1.90 ± 0.84 vs. 6.16 ± 1.44 vs. 6.30 ± 1.17, p < 0.001) and longer duration to regress to Bromage 0 (331.60 ± 73.96 vs. 185.56 ± 35.87 vs. 147.03 ± 33.05 min, p < 0.001), to analgesic request (496.63 ± 70.19 vs. 296.33 ± 44.83 vs. 221.83 ± 22.26 min, p < 0.001), to regress two sensory levels (149.00 ± 23.17 vs. 88.90 ± 12.85 vs. 69.33 ± 6.67 min, p < 0.001) and to regress to S1 (560.53 ± 81.86 vs. 329.83 ± 44.10 vs. 241.83 ± 22.26 min, p < 0.001). Serial changes in SBP (p = 0.006), DBP (p = 0.03) and HR (p = 0.002) in group BF were significantly higher than the other two groups. The three groups had comparable side effects.
Conclusions: Using dexmedetomidine as an adjuvant to bupivacaine for spinal anesthesia in lower limb surgeries has longer duration of sensory and motor block and longer postoperative analgesia.
Trial registration: IRCT registration number: IRCT2017041010599N15 , 24 May 2017.
Keywords: Dexmedetomidine; Fentanyl; Intrathecal; Lower limb surgery; Pain management.
Conflict of interest statement
Ethics approval and consent to participate
The Ethical Committee of Iran University of Medical Sciences approved the study and written informed consents were obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Elia N, Culebras X, Mazza C, Schiffer E, Tramèr MR. Clonidine as an adjuvant to intrathecal local anesthetics for surgery: systematic review of randomized trials. Reg Anesth Pain Med. 2008;33(2):159–167. - PubMed
-
- Shah A, Patel I, Gandhi R. Haemodynamic effects of intrathecal dexmedetomidine added to ropivacaine intraoperatively and for postoperative analgesia. Int J Basic Clin Pharmacol. 2013;2(1):26–29. doi: 10.5455/2319-2003.ijbcp20130105. - DOI
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
