

Arrhythmia-Induced Cardiomyopathy
- PMID: 29875055
- PMCID: PMC5997886
- DOI: 10.3238/arztebl.2018.0335
Arrhythmia-Induced Cardiomyopathy
Abstract
Background: Heart failure affects 1–2% of the population and is associated with elevated morbidity and mortality. Cardiac arrhythmias are often a result of heart failure, but they can cause left-ventricular systolic dysfunction (LVSD) as an arrhythmia-induced cardiomyopathy (AIC). This causal relationship should be borne in mind by the physician treating a patient with systolic heart failure in association with cardiac arrhythmia.
Methods: This review is based on pertinent publications retrieved by a selective search in PubMed (1987–2017) and on the recommendations in current guidelines.
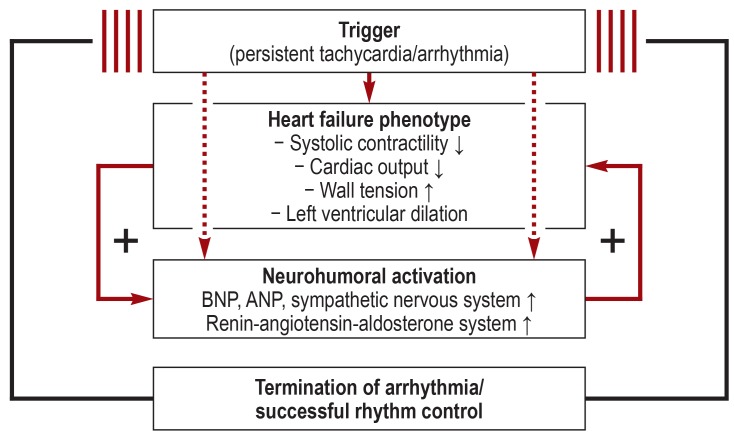
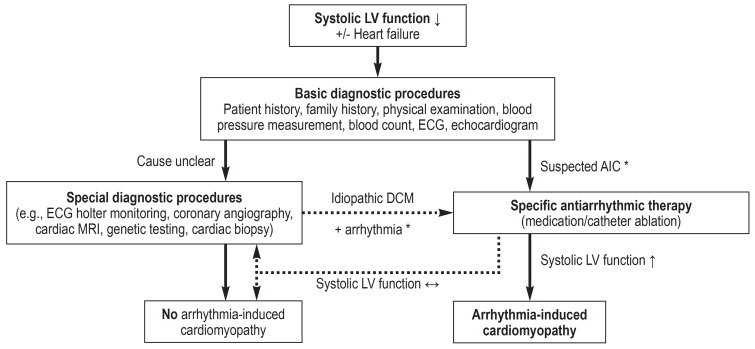
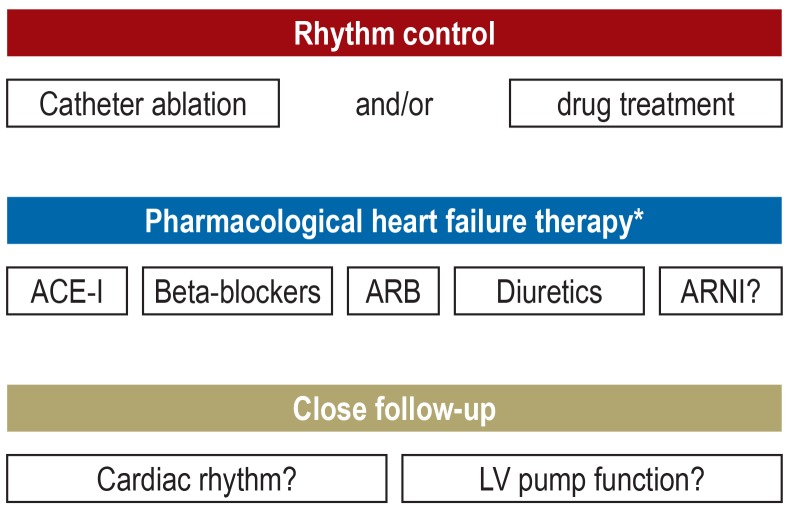
Results: The key criterion for the diagnosis of an AIC is the demonstration of a persistent arrhythmia (including pathological tachycardia) together with an LVSD whose origin cannot be explained on any other basis. Nearly any type of tachyarrhythmia or frequent ventricular extrasystoles can lead, if persistent, to a progressively severe LVSD. The underlying pathophysiologic mechanisms are incompletely understood; the increased ventricular rate, asynchronous cardiac contractions, and neurohumoral activation all seem to play a role. The most common precipitating factors are supraventricular tachycardias in children and atrial fibrillation in adults. Recent studies have shown that the causal significance of atrial fibrillation in otherwise unexplained LVSD is underappreciated. The treatment of AIC consists primarily of the treatment of the underlying arrhythmia, generally with drugs such as beta-blockers and amiodarone. Depending on the type of arrhythmia, catheter ablation for long-term treatment should also be considered where appropriate. The diagnosis of AIC is considered to be well established when the LVSD normalizes or improves within a few weeks or months of the start of targeted treatment of the arrhythmia.
Conclusion: An AIC is potentially reversible. The timely recognition of this condition and the appropriate treatment of the underlying arrhythmia can substantially improve patient outcomes.
Figures
Comment in
-
In Reply.Dtsch Arztebl Int. 2018 May 11;115(19):343-344. doi: 10.3238/arztebl.2018.0343. Dtsch Arztebl Int. 2018. PMID: 29875059 Free PMC article. No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. - PubMed
-
- van Riet EE, Hoes AW, Limburg A, Landman MA, van der Hoeven H, Rutten FH. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion. Eur J Heart Fail. 2014;16:772–777. - PubMed
-
- Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. - PubMed
-
- Bundesärztekammer (BÄK), KBK, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) Nationale VersorgungsLeitlinie Chronische Herzinsuffizienz - Langfassung Version 1 2017. DOI: 106101/AZQ/000386 2017.
-
- Santangeli P, Marzo F, Camporeale A, Bellocci F, Crea F, Pieroni M. What do tachycardiomyopathy belong to? Eur Heart J. 2008;29:1073–1074. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical