

Phase 2b study of 2 dosing regimens of quizartinib monotherapy in FLT3-ITD-mutated, relapsed or refractory AML
- PMID: 29875101
- PMCID: PMC6085992
- DOI: 10.1182/blood-2018-01-821629
Phase 2b study of 2 dosing regimens of quizartinib monotherapy in FLT3-ITD-mutated, relapsed or refractory AML
Abstract
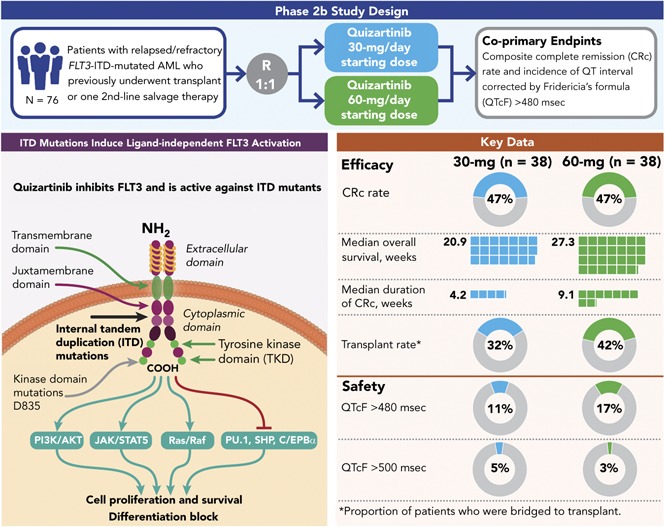
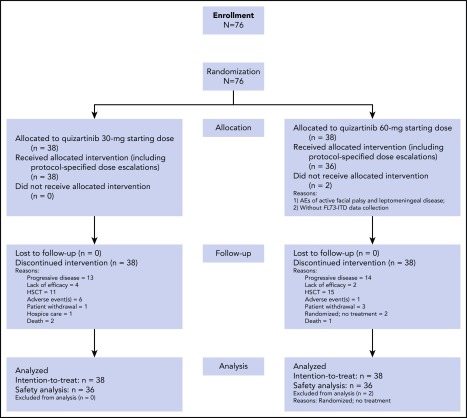
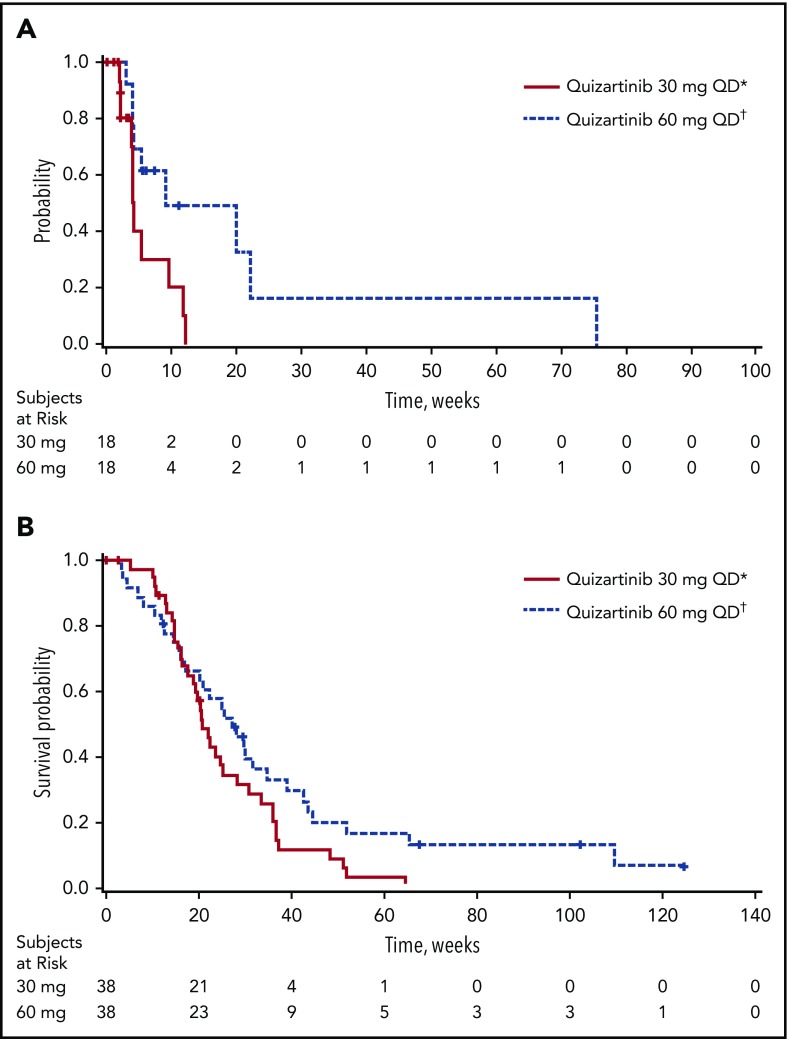
This randomized, open-label, phase 2b study (NCT01565668) evaluated the efficacy and safety of 2 dosing regimens of quizartinib monotherapy in patients with relapsed/refractory (R/R) FLT3-internal tandem duplication (ITD)-mutated acute myeloid leukemia (AML) who previously underwent transplant or 1 second-line salvage therapy. Patients (N = 76) were randomly assigned to 30- or 60-mg/day doses (escalations to 60 or 90 mg/day, respectively, permitted for lack/loss of response) of single-agent oral quizartinib dihydrochloride. Allelic frequency of at least 10% was defined as FLT3-ITD-mutated disease. Coprimary endpoints were composite complete remission (CRc) rates and incidence of QT interval corrected by Fridericia's formula (QTcF) of more than 480 ms (grade 2 or greater). Secondary endpoints included overall survival (OS), duration of CRc, bridge to transplant, and safety. CRc rates were 47% in both groups, similar to earlier reports with higher quizartinib doses. Incidence of QTcF above 480 ms was 11% and 17%, and QTcF above 500 ms was 5% and 3% in the 30- and 60-mg groups, respectively, which is less than earlier reports with higher doses of quizartinib. Median OS (20.9 and 27.3 weeks), duration of CRc (4.2 and 9.1 weeks), and bridge to transplant rates (32% and 42%) were higher in the 60-mg groups than in the 30-mg group. Dose escalation occurred in 61% and 14% of patients in the 30- and 60-mg groups, respectively. This high clinical activity of quizartinib at the evaluated doses is consistent with previous reports with an improved safety profile. Need to dose-escalate more than half of patients who received quizartinib 30 mg also supports further investigation of treatment with quizartinib 60 mg/day.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.E.C. is in a consulting or advisory role for Ambit, Daiichi Sankyo, Astellas, and Novartis and receives research funding (to his institution) from Ambit, Daiichi Sankyo, Astellas, AROG, Flexus, and Novartis. M.S.T. is in a consulting or advisory role for Daiichi Sankyo and receives research funding from AROG, Cellerant, ADC Therapeutics, and Celgene. G.J.S. receives research funding from Ambit. D.T. was employed by Daiichi Sankyo at the time of the conduct of this trial and is employed by Ambit Biosciences at this time. G.G. was employed by Daiichi Sankyo at the time of the conduct of this trial, is currently in a consulting or advisory role for Daiichi Sankyo (as chief executive officer of Guy Gammon Consulting), owns stock or other ownership in Daiichi Sankyo, and accepted travel provided with accommodations and reimbursement for expenses from Daiichi Sankyo. Current conflict-of-interest information for S.L.G. and A.E.P. may be found on the ASCO Web site. J.-P.M. receives honoraria from ICON Clinical. G.M. is in a consulting or advisory role with Celgene, Pfizer, Amgen, and Ariad and is on the speakers’ bureau for Incyte-Teva. H.M.K. receives honoraria from AbbVie, Actinium, Amgen, Ariad, BMS, Immunogen, Orsuex, and Pfizer and research funding (to his institution) from Amgen, Pfizer, Novartis, BMS, Astex, and Ariad. M.J.L. receives honoraria from Daiichi Sankyo, Novartis, and Agios, is in a consulting or advisory role for Daiichi Sankyo, Novartis, and Agios, and receives research funding from Astellas and Novartis.
Figures
References
-
- Kainz B, Heintel D, Marculescu R, et al. . Variable prognostic value of FLT3 internal tandem duplications in patients with de novo AML and a normal karyotype, t(15;17), t(8;21) or inv(16). Hematol J. 2002;3(6):283-289. - PubMed
-
- Kottaridis PD, Gale RE, Frew ME, et al. . The presence of a FLT3 internal tandem duplication in patients with acute myeloid leukemia (AML) adds important prognostic information to cytogenetic risk group and response to the first cycle of chemotherapy: analysis of 854 patients from the United Kingdom Medical Research Council AML 10 and 12 trials. Blood. 2001;98(6):1752-1759. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
