

Laboratory Diagnosis of Neurocysticercosis (Taenia solium)
- PMID: 29875195
- PMCID: PMC6113464
- DOI: 10.1128/JCM.00424-18
Laboratory Diagnosis of Neurocysticercosis (Taenia solium)
Abstract
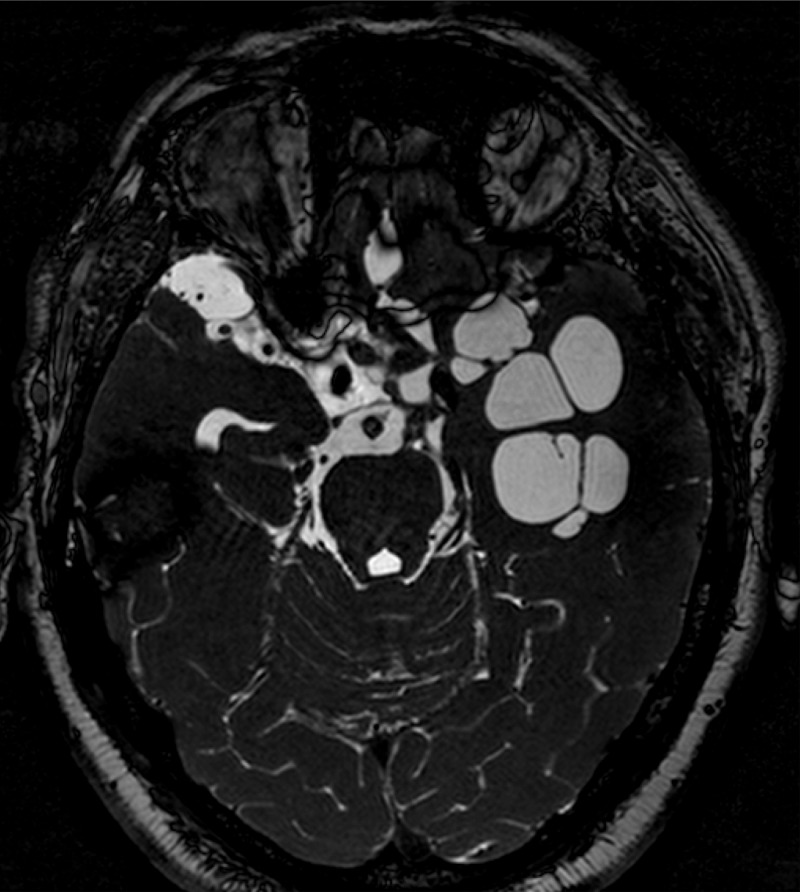
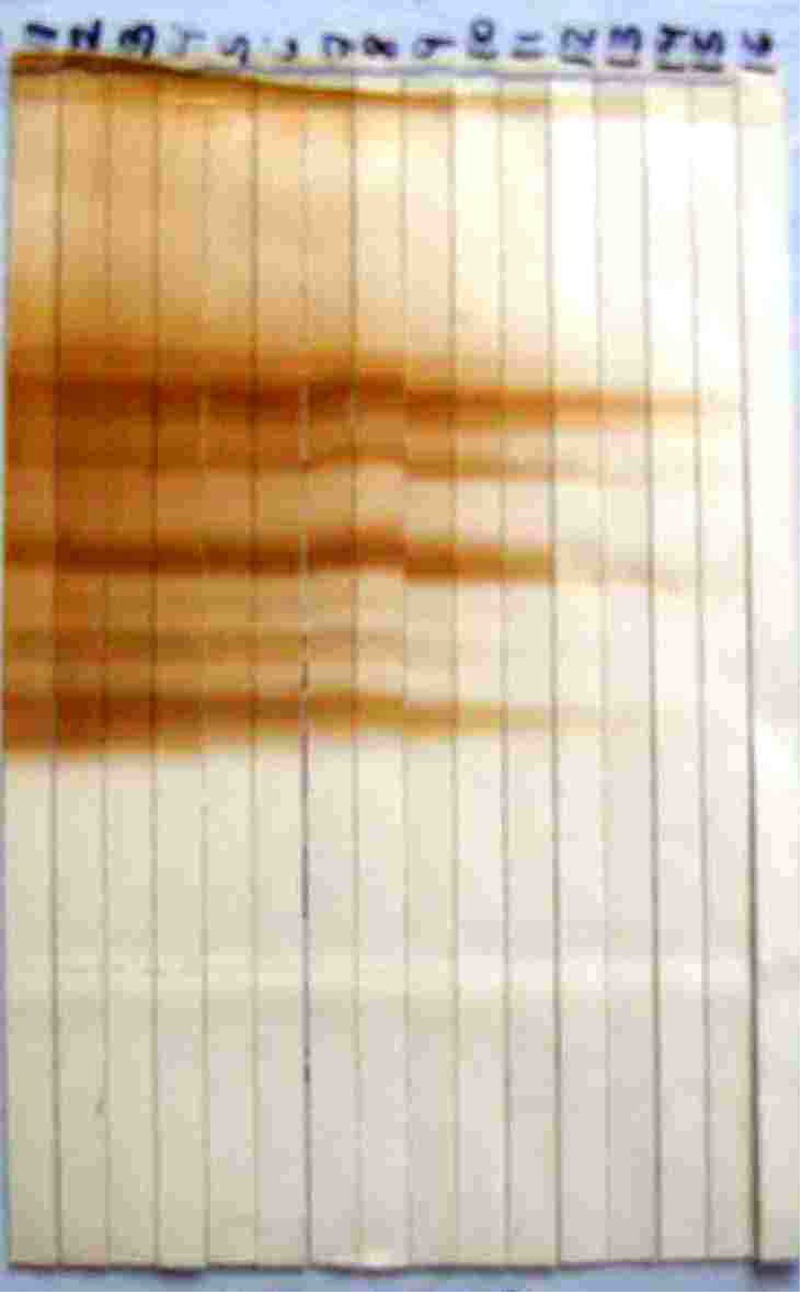
Neurocysticercosis accounts for approximately 30% of all epilepsy cases in most developing countries. The immunodiagnosis of cysticercosis is complex and strongly influenced by the course of infection, the disease burden, the cyst location, and the immune response of the host. The main approach to immunodiagnosis should thus be to evaluate whether the serological results are consistent with the diagnosis suggested by imaging. Antibody detection is performed using lentil lectin-purified parasite antigens in an enzyme-linked immunoelectrotransfer blot format, while antigen detection uses a monoclonal antibody-based enzyme-linked immunosorbent assay (ELISA). Promising new assay configurations have been developed for the detection of both antibody and antigen, including assays based on synthetic or recombinant antigens that may reduce costs and improve assay reproducibility and multiplex bead-based assays that may provide simultaneous quantitative results for several target antigens or antibodies.
Keywords: EITB; ELISA; Peru; Taenia solium; Western blot; antibody; antigen; cysticercosis; neurocysticercosis.
Copyright © 2018 American Society for Microbiology.
Figures

References
-
- Yoshino K. 1933. Studies on the post-embryonal development of Taenia solium: III. On the development of Cysticercus cellulosae within the definitive intermediate host. J Med Assoc Formosa 32:166–169.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
