

Internal Hernia in Pregnant Woman after Roux-en-Y Gastric Bypass Surgery
- PMID: 29875982
- PMCID: PMC5965396
- DOI: 10.3941/jrcr.v12i1.3257
Internal Hernia in Pregnant Woman after Roux-en-Y Gastric Bypass Surgery
Abstract
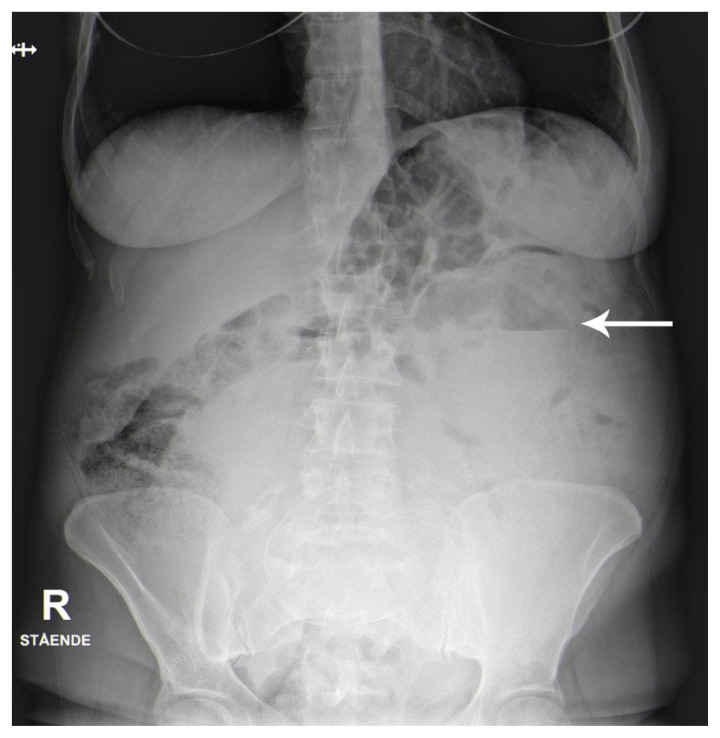
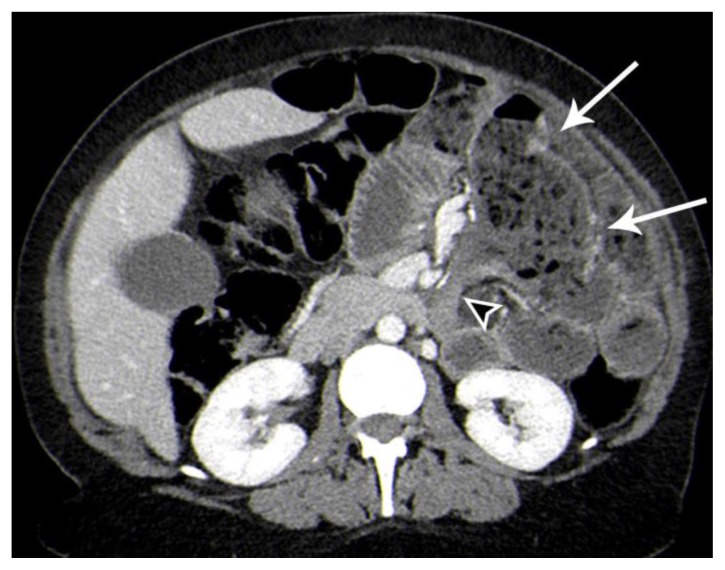
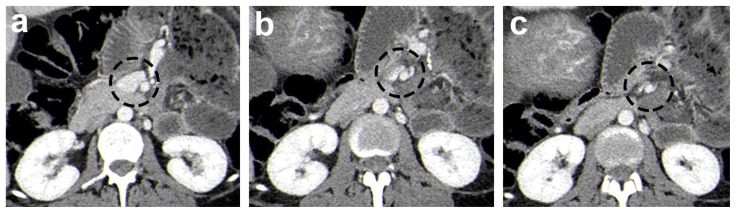
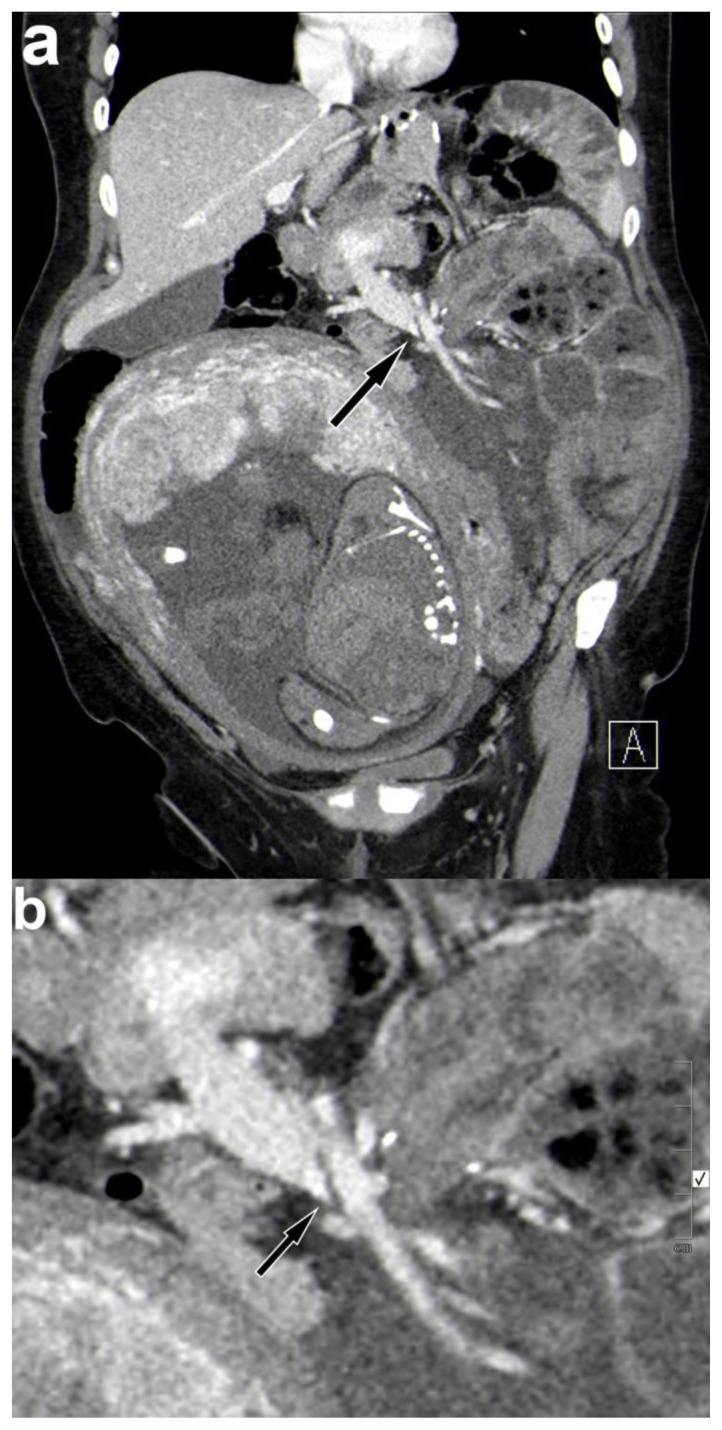
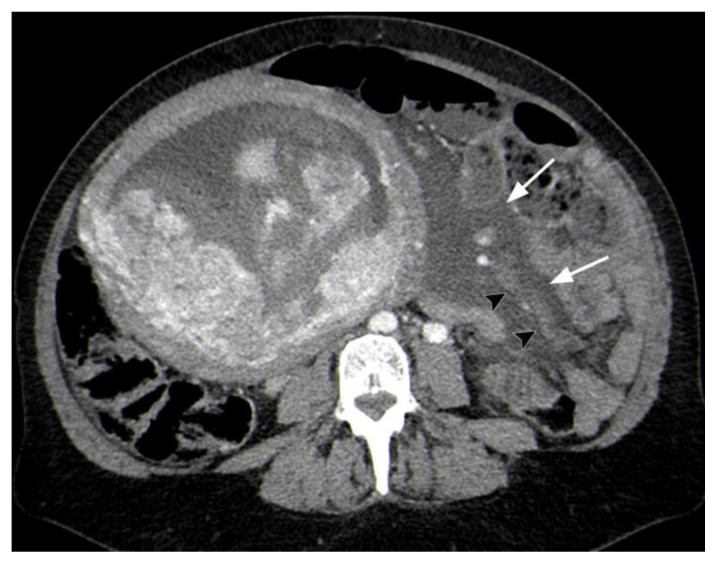
Laparoscopic Roux-en-Y gastric bypass has become the most common obesity surgery procedure worldwide over the last two decades. Many patients undergoing the procedure are women of reproductive age. This carries a risk for developing gastric bypass-related complications during pregnancy. One of the potentially serious risks is an internal hernia. We present a patient in the third trimester of pregnancy with an internal hernia following a laparoscopic Roux-en-Y gastric bypass for morbid obesity. We discuss the importance of computed tomography (CT) in the diagnosis of an internal hernia and review key CT findings including compression of the superior mesenteric vein, which proved to be crucial in diagnosing the internal hernia in this patient.
Keywords: CT scan; Gastric bypass; Roux-en-Y gastric bypass; SMV beaking sign; SMV compression; internal hernia; pregnancy; swirl sign.
Figures
Similar articles
-
Internal Hernia after Laparoscopic Roux-en-Y Gastric Bypass: Optimal CT Signs for Diagnosis and Clinical Decision Making.Radiology. 2017 Mar;282(3):752-760. doi: 10.1148/radiol.2016160956. Epub 2016 Sep 30. Radiology. 2017. PMID: 27689925
-
Compression of the superior mesenteric vein-a sign of acute internal herniation in patients with antecolic laparoscopic Roux-en-Y gastric bypass.Eur Radiol. 2017 Apr;27(4):1733-1739. doi: 10.1007/s00330-016-4526-9. Epub 2016 Aug 9. Eur Radiol. 2017. PMID: 27507304
-
The diagnostic performance and interrater agreement of seven CT findings in the diagnosis of internal hernia after gastric bypass operation.Abdom Radiol (NY). 2018 Dec;43(12):3220-3226. doi: 10.1007/s00261-018-1640-y. Abdom Radiol (NY). 2018. PMID: 29845311
-
Re-do Roux-en-Y gastric bypass in a patient with known midgut malrotation.JSLS. 2013 Jul-Sep;17(3):463-7. doi: 10.4293/108680813x13753907291990. JSLS. 2013. PMID: 24018088 Free PMC article. Review.
-
Computed Tomography of Internal Hernias Following Laparoscopic Roux-en-Y Gastric Bypass Surgery.Semin Ultrasound CT MR. 2018 Apr;39(2):145-150. doi: 10.1053/j.sult.2017.11.002. Epub 2017 Nov 14. Semin Ultrasound CT MR. 2018. PMID: 29571551 Review.
Cited by
-
Internal Hernia in Pregnant Woman due to Congenital Transmesenteric Defect.Pak J Med Sci. 2021 Sep-Oct;37(5):1540-1544. doi: 10.12669/pjms.37.5.4116. Pak J Med Sci. 2021. PMID: 34475945 Free PMC article.
-
Management of small bowel obstruction in the third trimester.BMJ Case Rep. 2024 Mar 5;17(3):e255843. doi: 10.1136/bcr-2023-255843. BMJ Case Rep. 2024. PMID: 38442967
-
How to Treat Hernias in Pregnant Women?Cureus. 2020 Jul 2;12(7):e8959. doi: 10.7759/cureus.8959. Cureus. 2020. PMID: 32766002 Free PMC article. Review.
-
Internal hernia through the mesenteric defect in twin pregnancy: a case report and literature review.Front Med (Lausanne). 2024 Nov 29;11:1479634. doi: 10.3389/fmed.2024.1479634. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39678031 Free PMC article.
References
-
- Andreasen LA, Nilas L, Kjær MM. Operative complications during pregnancy after gastric bypass-a register-based cohort study. Obes Surg. 2014;24:1634–1638. - PubMed
-
- Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic gastric bypass, Roux-en-Y: Preliminary report of five cases. Obes Surg. 1994 Nov;4(4):353–357. - PubMed
-
- Scheirey CD, Scholz FJ, Shah PC, Brams DM, Wong BB, Pedrosa M. Radiology of the laparoscopic Roux-en-Y gastric bypass procedure: conceptualization and precise interpretation of results. Radiographics. 2006;26(5):1355–71. - PubMed
-
- Goudsmedt F, Deylgat B, Coenegrachts K, Van De Moortele K, Dillemans B. Internal hernia after laparoscopic Roux-en-Y gastric bypass: a correlation between radiological and operative findings. Obes Surg. 2015;25(4):622–627. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials