

Pulmonary Hypertension in Aortic and Mitral Valve Disease
- PMID: 29876357
- PMCID: PMC5974123
- DOI: 10.3389/fcvm.2018.00040
Pulmonary Hypertension in Aortic and Mitral Valve Disease
Abstract
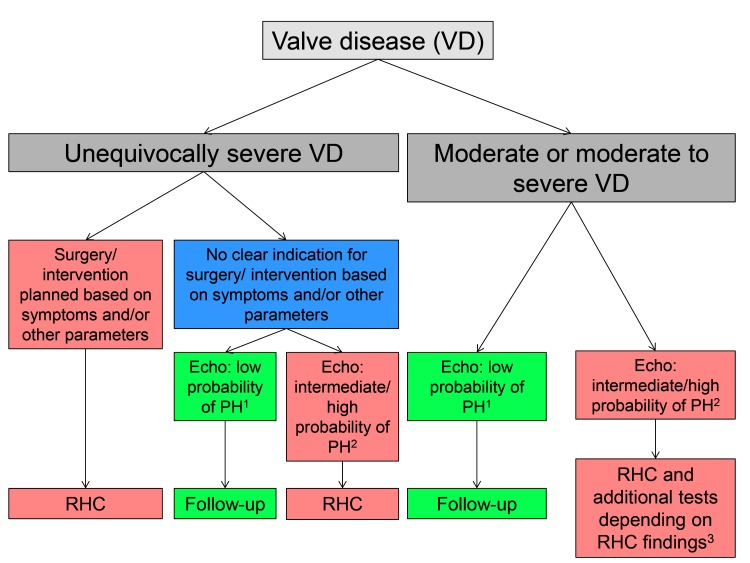
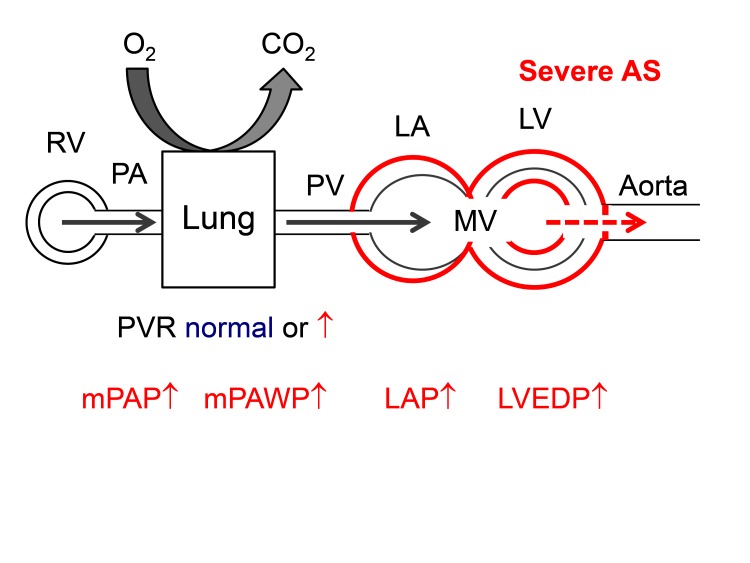
In patients with aortic and/or mitral valve disease the presence of pulmonary hypertension (PH) indicates a decompensated state of the disease with left ventricular and left atrial dysfunction and exhausted compensatory mechanism, i.e., a state of heart failure. Pulmonary hypertension in this context is the consequence of the backwards transmission of elevated left atrial pressure. In this form of PH, pulmonary vascular resistance is initially normal (isolated post-capillary PH). Depending on the extent and chronicity of left atrial pressure elevation additional pulmonary vascular remodeling may occur (combined pre- and post-capillary PH). Mechanical interventions for the correction of valve disease often but not always reduce pulmonary pressures. However, the reduction in pulmonary pressures is often modest, and persistent PH in these patients is common and a marker of poor prognosis. In the present review we discuss the pathophysiology and clinical impact of PH in patients with aortic and mitral valve disease, the comprehensive non-invasive and invasive diagnostic approach required to define treatment of PH, and recent insights from mechanistic studies, registries and randomized studies, and we provide an outlook regarding gaps in evidence, future clinical challenges, and research opportunities in this setting.
Keywords: aortic stenosis; combined pre- and post-capillary; mitral regurgitation; post-capillary; pre-capillary; pulmonary hypertension; valve disease.
Figures






References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J (2016) 37(1):67–119. 10.1093/eurheartj/ehv317 - DOI - PubMed
-
- Fawzy ME, Osman A, Nambiar V, Nowayhed O, El DA, Badr A, et al. Immediate and long-term results of mitral balloon valvuloplasty in patients with severe pulmonary hypertension. J Heart Valve Dis (2008) 17(5):485–91. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources