

Machine-learning-derived classifier predicts absence of persistent pain after breast cancer surgery with high accuracy
- PMID: 29876695
- PMCID: PMC6096884
- DOI: 10.1007/s10549-018-4841-8
Machine-learning-derived classifier predicts absence of persistent pain after breast cancer surgery with high accuracy
Abstract
Background: Prevention of persistent pain following breast cancer surgery, via early identification of patients at high risk, is a clinical need. Supervised machine-learning was used to identify parameters that predict persistence of significant pain.
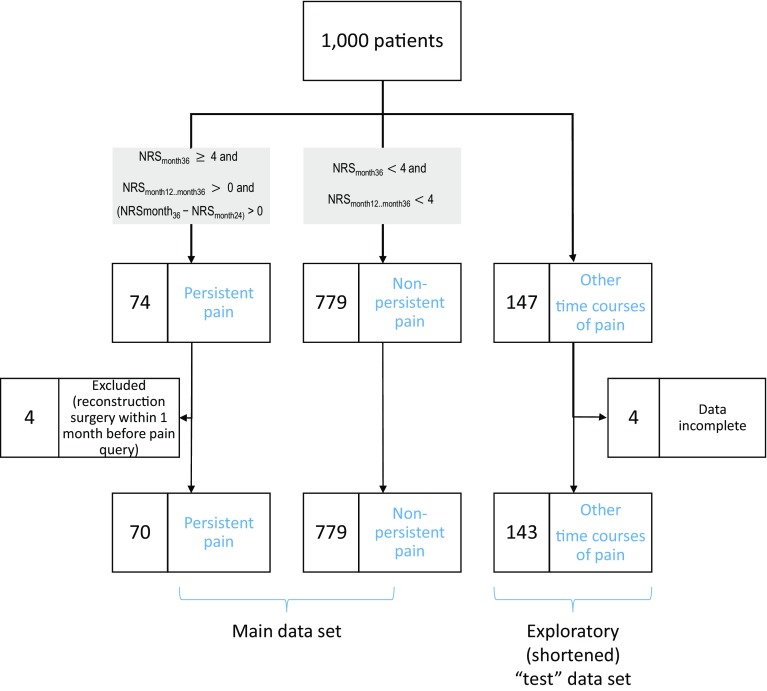
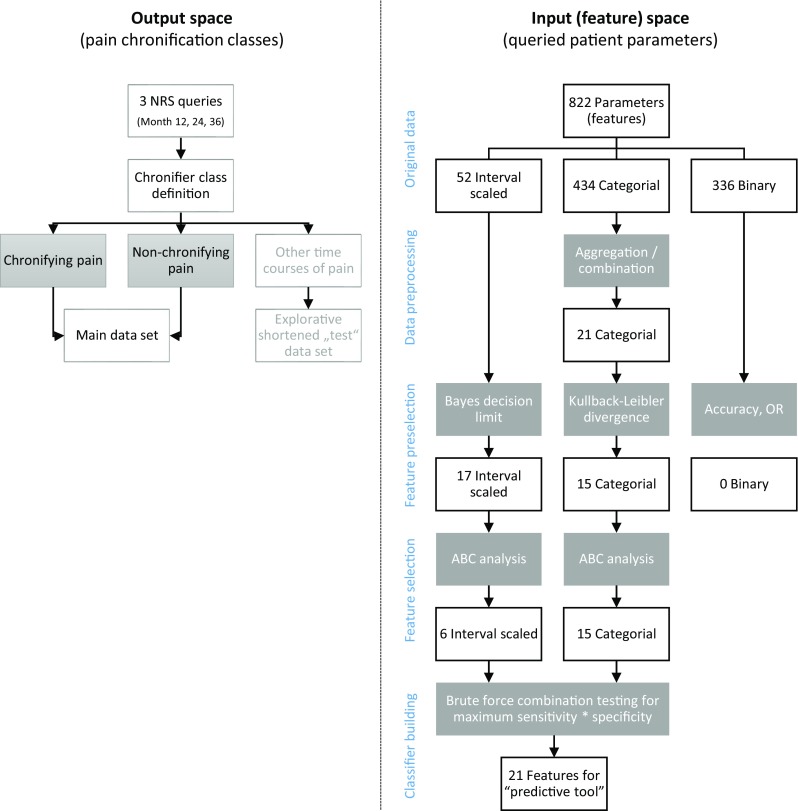
Methods: Over 500 demographic, clinical and psychological parameters were acquired up to 6 months after surgery from 1,000 women (aged 28-75 years) who were treated for breast cancer. Pain was assessed using an 11-point numerical rating scale before surgery and at months 1, 6, 12, 24, and 36. The ratings at months 12, 24, and 36 were used to allocate patents to either "persisting pain" or "non-persisting pain" groups. Unsupervised machine learning was applied to map the parameters to these diagnoses.
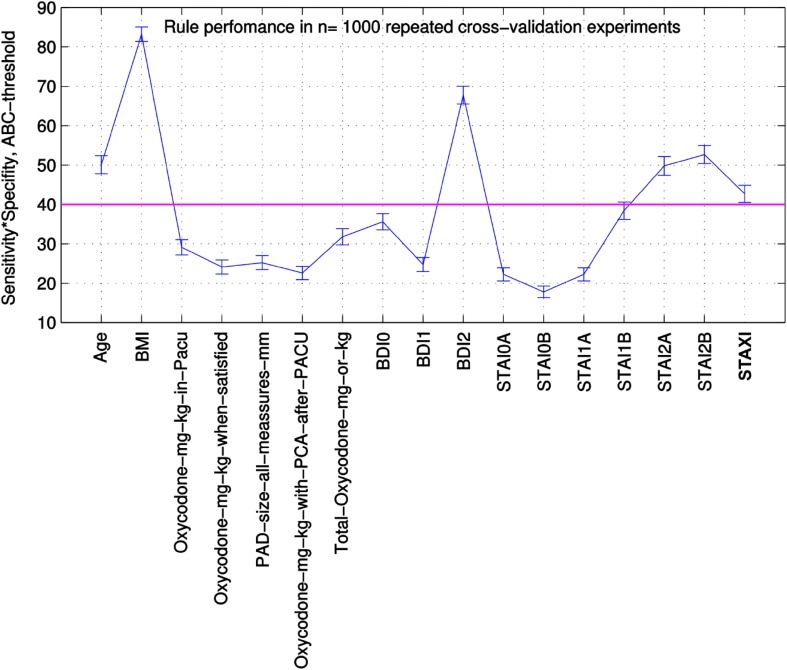
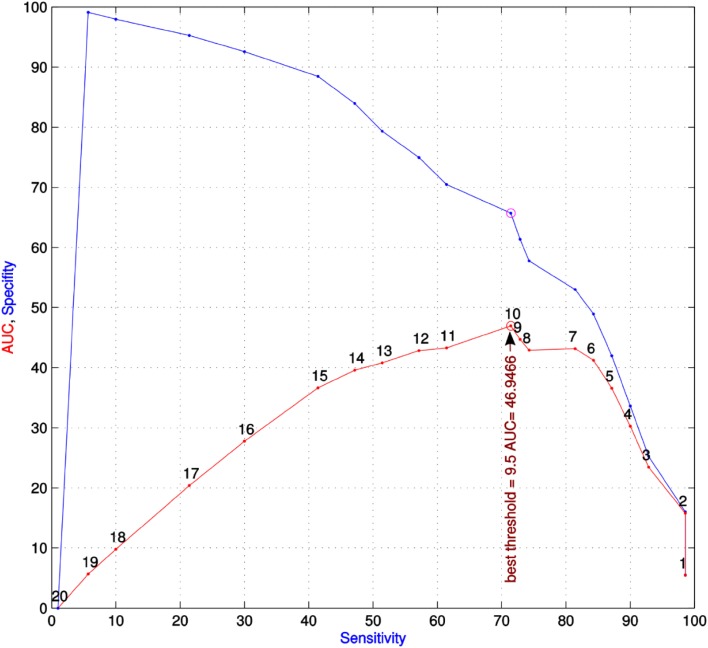
Results: A symbolic rule-based classifier tool was created that comprised 21 single or aggregated parameters, including demographic features, psychological and pain-related parameters, forming a questionnaire with "yes/no" items (decision rules). If at least 10 of the 21 rules applied, persisting pain was predicted at a cross-validated accuracy of 86% and a negative predictive value of approximately 95%.
Conclusions: The present machine-learned analysis showed that, even with a large set of parameters acquired from a large cohort, early identification of these patients is only partly successful. This indicates that more parameters are needed for accurate prediction of persisting pain. However, with the current parameters it is possible, with a certainty of almost 95%, to exclude the possibility of persistent pain developing in a woman being treated for breast cancer.
Keywords: Bioinformatics; Chronification; Data science; Pain.
Conflict of interest statement
The authors have declared no competing interests.
Figures
References
-
- Bruce J, Thornton AJ, Scott NW, Marfizo S, Powell R, Johnston M, Wells M, Heys SD, Thompson AM. Chronic preoperative pain and psychological robustness predict acute postoperative pain outcomes after surgery for breast cancer. Br J Cancer. 2012;107:937–946. doi: 10.1038/bjc.2012.341. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
