

Visual Acuity Is Not the Best at the Preferred Retinal Locus in People with Macular Disease
- PMID: 29877902
- PMCID: PMC6119096
- DOI: 10.1097/OPX.0000000000001229
Visual Acuity Is Not the Best at the Preferred Retinal Locus in People with Macular Disease
Abstract
Significance: Little is known about how the preferred retinal locus (PRL) develops in patients with macular disease. We found that acuity is worse at the PRL than at other retinal locations around the scotoma, suggesting that the selection of the PRL location is unlikely to be based on optimizing acuity.
Purpose: Following the onset of bilateral macular disease, most patients adopt a retinal location outside the central scotoma, the PRL, as their new retinal location for visual tasks. Very little information is known about how the location of a PRL is chosen. In this study, we tested the hypothesis that the selection of the location for a PRL is based on optimizing visual acuity, which predicts that acuity is the best at the PRL, compared with other retinal locations.
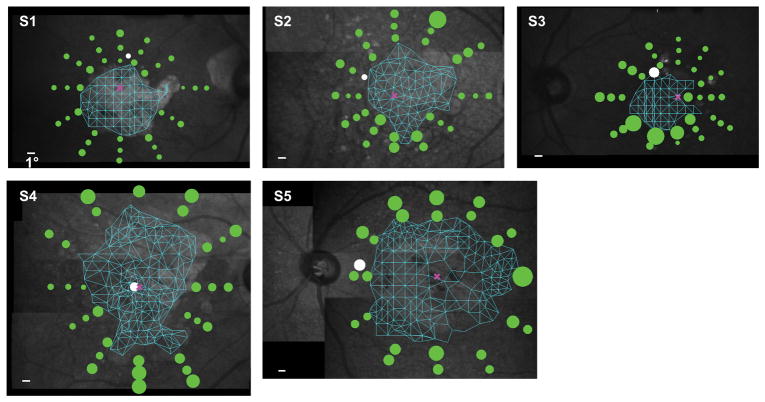
Methods: Using a scanning laser ophthalmoscope that allowed us to position visual targets at precise retinal locations, we measured acuity psychophysically using a four-orientation Tumbling-E presented at the PRL and at multiple (ranged between 23 and 36 across observers) locations around the scotoma for five observers with bilateral macular disease.
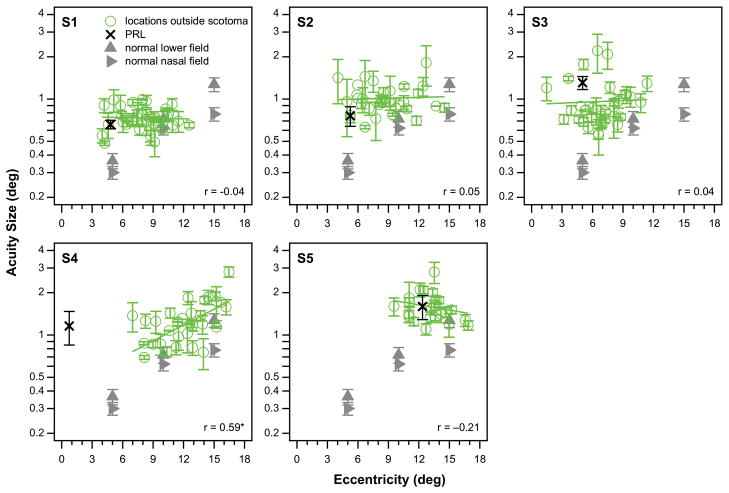
Results: For all five observers, the acuity at the PRL was never the best among all testing locations. Instead, acuities were better at 15 to 86% of the testing locations other than the PRL, with the best acuity being 17 to 58% better than that at the PRL. The locations with better acuities did not cluster around the PRL and did not necessarily lie at the same distance from the fovea or the PRL.
Conclusions: Our finding that acuity is worse at the PRL than at other locations around the scotoma implies that the selection of the PRL location is unlikely to be based on optimizing acuity.
Figures



Comment in
-
Letter to the Editor: Visual Acuity Is Not the Best at the Preferred Retinal Locus in People with Macular Disease.Optom Vis Sci. 2019 Feb;96(2):142. doi: 10.1097/OPX.0000000000001340. Optom Vis Sci. 2019. PMID: 30707208 No abstract available.
-
Authors' Response.Optom Vis Sci. 2019 Feb;96(2):143. doi: 10.1097/OPX.0000000000001341. Optom Vis Sci. 2019. PMID: 30707209 Free PMC article. No abstract available.
References
-
- Cummings RW, Whittaker SG, Watson GR, Budd JM. Scanning Characters and Reading with a Central Scotoma. Am J Optom Physiol Opt. 1985;62:833–43. - PubMed
-
- Timberlake GT, Mainster MA, Peli E, et al. Reading with a Macular Scotoma. I. Retinal Location of Scotoma and Fixation Area. Invest Ophthalmol Vis Sci. 1986;27:1137–47. - PubMed
-
- Lei H, Schuchard RA. Using Two Preferred Retinal Loci for Different Lighting Conditions in Patients with Central Scotomas. Invest Ophthalmol Vis Sci. 1997;38:1812–8. - PubMed
-
- Crossland MD, Crabb DP, Rubin GS. Task-Specific Fixation Behavior in Macular Disease. Invest Ophthalmol Vis Sci. 2011;52:411–6. - PubMed
-
- Duret F, Issenhuth M, Safran A. Combined Use of Several Preferred Retinal Loci in Patients with Macular Disorders when Reading Single Words. Vision Res. 1999;39:873–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
