

Estimation of the maternal vitamin D intake that maintains circulating 25-hydroxyvitamin D in late gestation at a concentration sufficient to keep umbilical cord sera ≥25-30 nmol/L: a dose-response, double-blind, randomized placebo-controlled trial in pregnant women at northern latitude
- PMID: 29878035
- PMCID: PMC6600055
- DOI: 10.1093/ajcn/nqy064
Estimation of the maternal vitamin D intake that maintains circulating 25-hydroxyvitamin D in late gestation at a concentration sufficient to keep umbilical cord sera ≥25-30 nmol/L: a dose-response, double-blind, randomized placebo-controlled trial in pregnant women at northern latitude
Abstract
Background: In the absence of dose-response data, Dietary Reference Values for vitamin D in nonpregnant adults are extended to pregnancy.
Objective: The aim was to estimate vitamin D intake needed to maintain maternal 25-hydroxyvitamin D [25(OH)D] in late gestation at a concentration sufficient to prevent newborn 25(OH)D <25-30 nmol/L, a threshold indicative of increased risk of nutritional rickets.
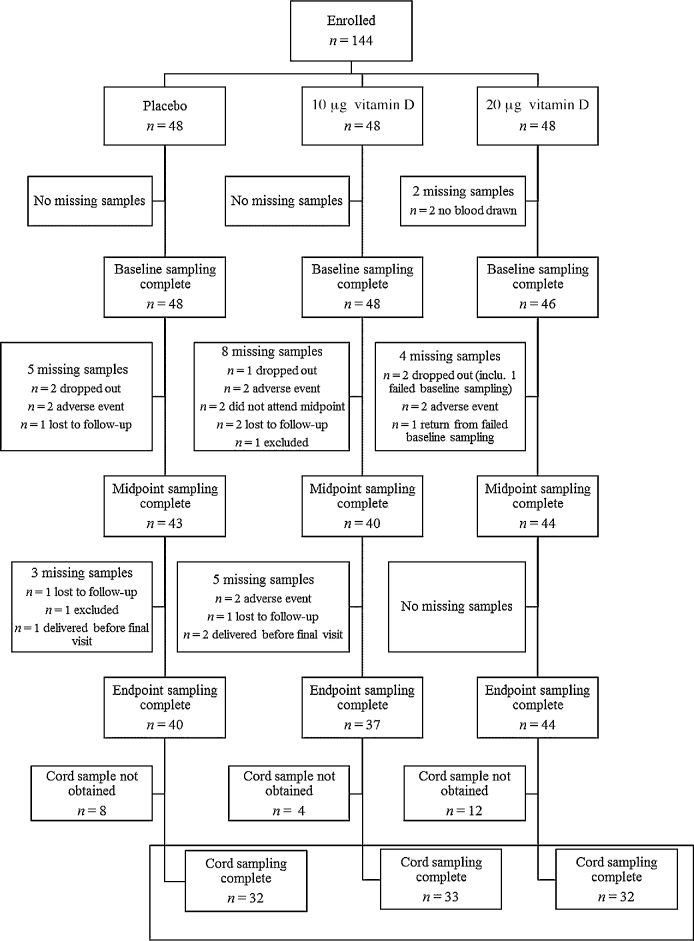
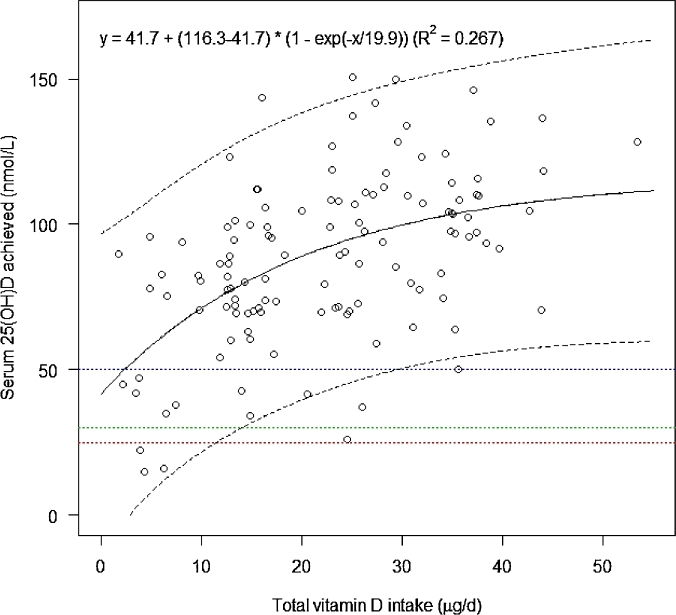
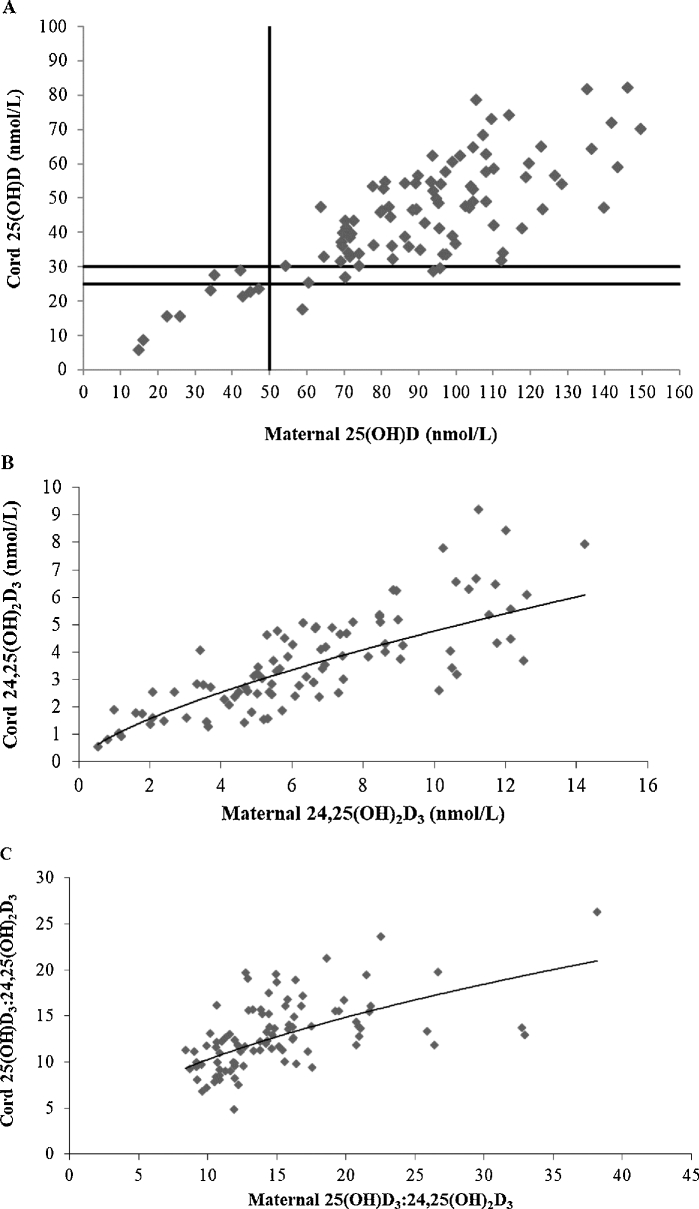
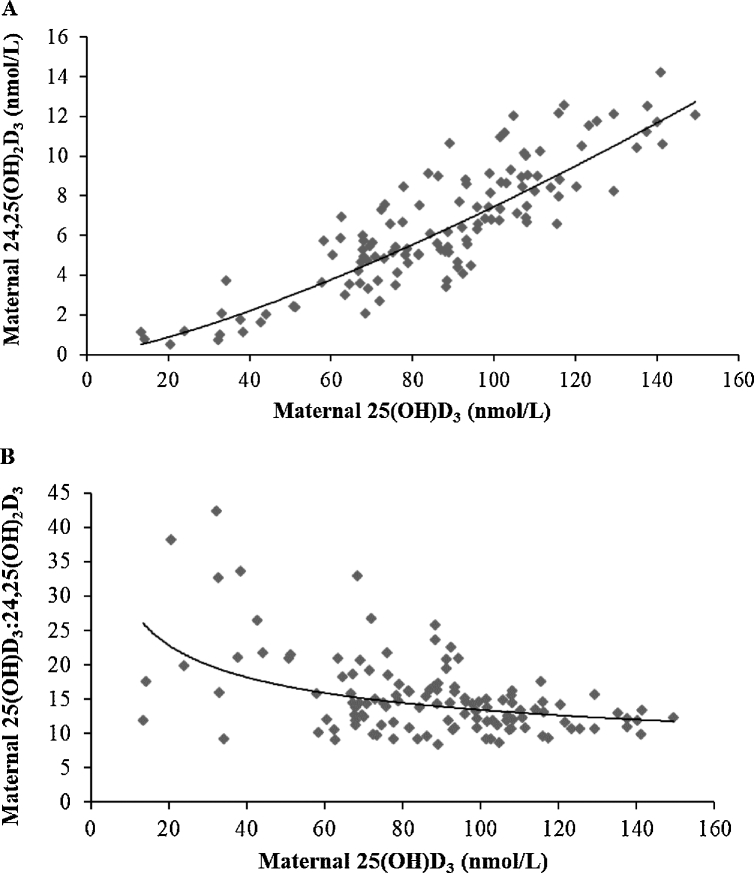
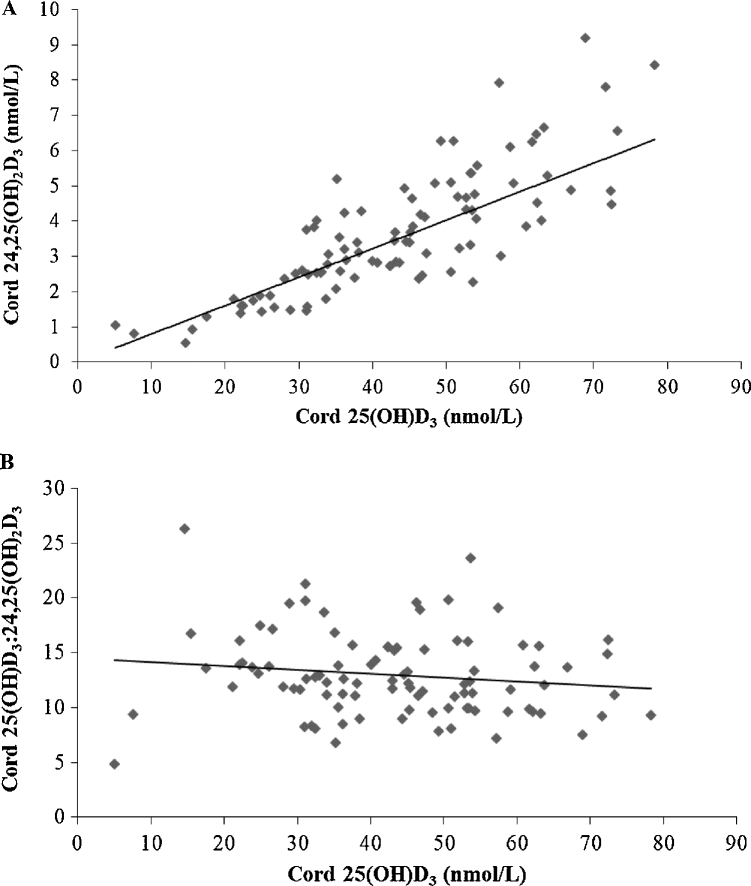
Design: We conducted a 3-arm, dose-response, double-blind, randomized placebo-controlled trial in Cork, Ireland (51.9oN). A total of 144 white-skinned pregnant women were assigned to receive 0, 10 (400 IU), or 20 (800 IU) µg vitamin D3/d from ≤18 wk of gestation. Vitamin D metabolites at 14, 24, and 36 wk of gestation and in cord sera, including 25(OH)D3, 3-epi-25(OH)D3, 24,25(OH)2D3, and 25(OH)D2 were quantified by liquid chromatography-tandem mass spectrometry. A curvilinear regression model predicted the total vitamin D intake (from diet and antenatal supplements plus treatment dose) that maintained maternal 25(OH)D in late gestation at a concentration sufficient to maintain cord 25(OH)D at ≥25-30 nmol/L.
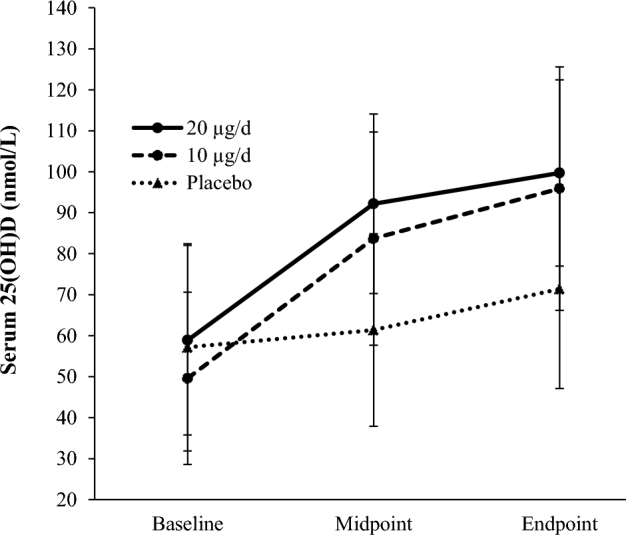
Results: Mean ± SD baseline 25(OH)D was 54.9 ± 10.7 nmol/L. Total vitamin D intakes at the study endpoint (36 wk of gestation) were 12.1 ± 8.0, 21.9 ± 5.3, and 33.7 ± 5.1 µg/d in the placebo and 10-µg and 20-µg vitamin D3 groups, respectively; and 25(OH)D was 24.3 ± 5.8 and 29.2 ± 5.6 nmol/L higher in the 10- and 20-µg groups, respectively, compared with placebo (P < 0.001). For maternal 25(OH)D concentrations ≥50 nmol/L, 95% of cord sera were ≥30 nmol/L and 99% were >25 nmol/L. The estimated vitamin D intake required to maintain serum 25(OH)D at ≥50 nmol/L in 97.5% of women was 28.9 µg/d.
Conclusions: Thirty micrograms of vitamin D per day safely maintained serum 25(OH)D concentrations at ≥50 nmol/L in almost all white-skinned women during pregnancy at a northern latitude, which kept 25(OH)D at >25 nmol/L in 99% and ≥30 nmol/L in 95% of umbilical cord sera. This trial was registered at www.clinicaltrials.gov as NCT02506439.
Figures

References
-
- Institute of Medicine Dietary Reference Intakes for calcium and vitamin D. Washington (DC): National Academies Press; 2011. - PubMed
-
- Nordic Council of Ministers Nordic Nutrition Recommendations 2012: integrating nutrition and physical activity. Copenhagen (Denmark): Nordic Council of Ministers; 2012.
-
- Scientific Advisory Committee on Nutrition Vitamin D and health. London: The Stationary Office; 2016.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
