

Revealing Measles Outbreak Risk With a Nested Immunoglobulin G Serosurvey in Madagascar
- PMID: 29878051
- PMCID: PMC6166215
- DOI: 10.1093/aje/kwy114
Revealing Measles Outbreak Risk With a Nested Immunoglobulin G Serosurvey in Madagascar
Abstract
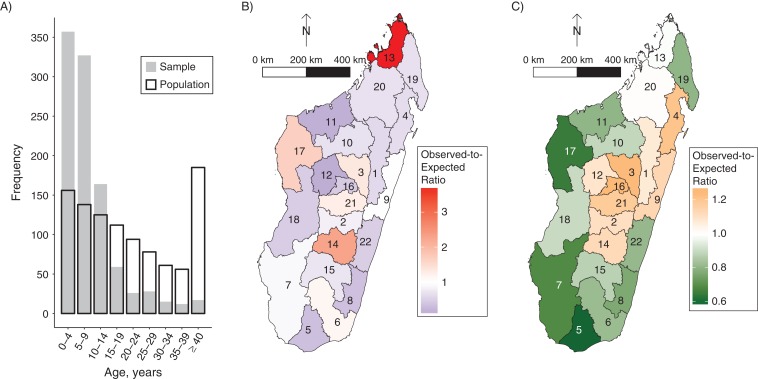
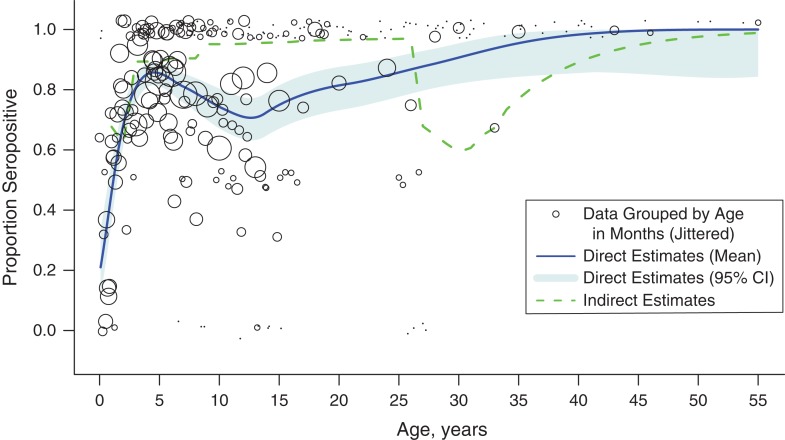
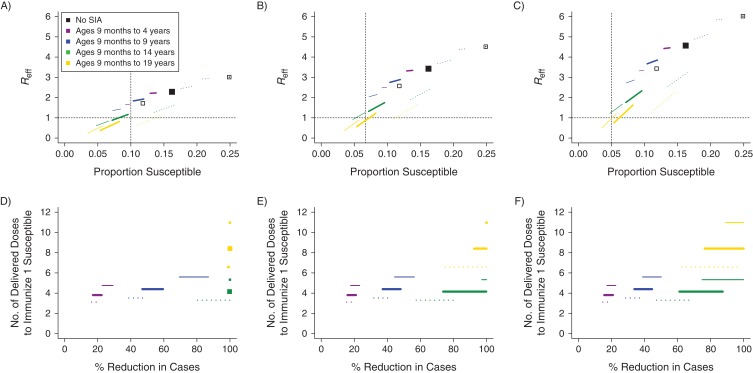
Madagascar reports few measles cases annually and high vaccination campaign coverage. However, the underlying age profile of immunity and risk of a measles outbreak is unknown. We conducted a nested serological survey, testing 1,005 serum samples (collected between November 2013 and December 2015 via Madagascar's febrile rash surveillance system) for measles immunoglobulin G antibody titers. We directly estimated the age profile of immunity and compared these estimates with indirect estimates based on a birth cohort model of vaccination coverage and natural infection. Combining these estimates of the age profile of immunity in the population with an age-structured model of transmission, we further predicted the risk of a measles outbreak and the impact of mitigation strategies designed around supplementary immunization activities. The direct and indirect estimates of age-specific seroprevalence show that current measles susceptibility is over 10%, and modeling suggests that Madagascar may be at risk of a major measles epidemic.
Figures
Similar articles
-
Measles and rubella serosurvey identifies rubella immunity gap in young adults of childbearing age in Zambia: The added value of nesting a serological survey within a post-campaign coverage evaluation survey.Vaccine. 2019 Apr 17;37(17):2387-2393. doi: 10.1016/j.vaccine.2019.02.037. Epub 2019 Mar 21. Vaccine. 2019. PMID: 30905529 Free PMC article.
-
Evaluation of nationwide supplementary immunization in Lao People's Democratic Republic: Population-based seroprevalence survey of anti-measles and anti-rubella IgG in children and adults, mathematical modelling and a stability testing of the vaccine.PLoS One. 2018 Mar 29;13(3):e0194931. doi: 10.1371/journal.pone.0194931. eCollection 2018. PLoS One. 2018. PMID: 29596472 Free PMC article.
-
Measles seroprevalence, outbreaks, and vaccine coverage in Rwanda.Infect Dis (Lond). 2016 Nov-Dec;48(11-12):800-7. doi: 10.1080/23744235.2016.1201720. Epub 2016 Jul 8. Infect Dis (Lond). 2016. PMID: 27386895
-
[Vaccination coverage against measles and sero-epidemiology of measles-specific IgG antibodies in German children and adolescents].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013 Sep;56(9):1243-52. doi: 10.1007/s00103-013-1790-6. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013. PMID: 23990086 Review. German.
-
A 16-year review of seroprevalence studies on measles and rubella.Vaccine. 2016 Jul 29;34(35):4110-4118. doi: 10.1016/j.vaccine.2016.06.002. Epub 2016 Jun 20. Vaccine. 2016. PMID: 27340097 Review.
Cited by
-
Towards better targeting: lessons from a posthoneymoon measles outbreak in Madagascar, 2018-2019.BMJ Glob Health. 2020 Oct;5(10):e003153. doi: 10.1136/bmjgh-2020-003153. BMJ Glob Health. 2020. PMID: 33082133 Free PMC article. No abstract available.
-
Using models to shape measles control and elimination strategies in low- and middle-income countries: A review of recent applications.Vaccine. 2020 Jan 29;38(5):979-992. doi: 10.1016/j.vaccine.2019.11.020. Epub 2019 Nov 29. Vaccine. 2020. PMID: 31787412 Free PMC article. Review.
-
Leveraging a national biorepository in Zambia to assess measles and rubella immunity gaps across age and space.Sci Rep. 2022 Jun 17;12(1):10217. doi: 10.1038/s41598-022-14493-3. Sci Rep. 2022. PMID: 35715547 Free PMC article.
-
The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections.Proc Natl Acad Sci U S A. 2020 Dec 1;117(48):30547-30553. doi: 10.1073/pnas.2013182117. Epub 2020 Nov 9. Proc Natl Acad Sci U S A. 2020. PMID: 33168723 Free PMC article.
-
The Use of Residual Blood Specimens in Seroprevalence Studies for Vaccine-Preventable Diseases: A Scoping Review.Vaccines (Basel). 2025 Mar 18;13(3):321. doi: 10.3390/vaccines13030321. Vaccines (Basel). 2025. PMID: 40266228 Free PMC article. Review.
References
-
- Plotkin S, Orenstein W, Offit P eds. Vaccines. 6th ed Philadelphia, PA: Elsvier; 2013.
-
- World Health Organization Measles vaccines: WHO position paper. Wkly Epidemiol Rec. 2009;84(35):349–360. - PubMed
-
- World Health Organization Data, statistics and graphics, 4.5: WHO/UNICEF Estimates of National Immunization Coverage (WUENIC) [estimates for 1980 to 2016]. http://www.who.int/immunization/monitoring_surveillance/data/en/. Accessed May 21, 2018.
-
- World Health Organization Data, statistics and graphics: Retrospective Measles Data on Supplementary Immunization Activities, 2000–2015. http://www.who.int/immunization/monitoring_surveillance/data/en/. Accessed May 21, 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
