

Variation in antibiotic use among and within different settings: a systematic review
- PMID: 29878219
- PMCID: PMC5989604
- DOI: 10.1093/jac/dky115
Variation in antibiotic use among and within different settings: a systematic review
Abstract
Objectives: Variation in antibiotic use may reflect inappropriate use. We aimed to systematically describe the variation in measures for antibiotic use among settings or providers. This study was conducted as part of the innovative medicines initiative (IMI)-funded international project DRIVE-AB.
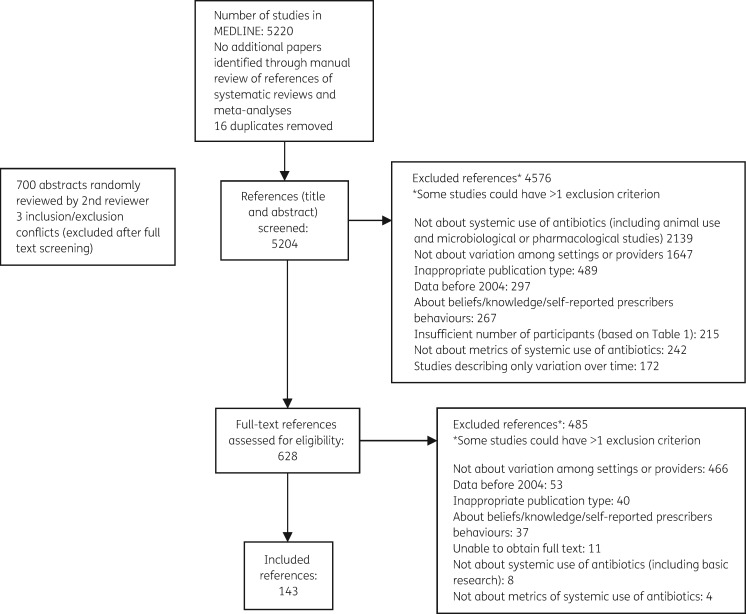
Methods: We searched for studies published in MEDLINE from January 2004 to January 2015 reporting variation in measures for systemic antibiotic use (e.g. DDDs) in inpatient and outpatient settings. The ratio between a study's reported maximum and minimum values of a given measure [maximum:minimum ratio (MMR)] was calculated as a measure of variation. Similar measures were grouped into categories and when possible the overall median ratio and IQR were calculated.
Results: One hundred and forty-three studies were included, of which 85 (59.4%) were conducted in Europe and 12 (8.4%) in low- to middle-income countries. Most studies described the variation in the quantity of antibiotic use in the inpatient setting (81/143, 56.6%), especially among hospitals (41/81, 50.6%). The most frequent measure was DDDs with different denominators, reported in 23/81 (28.4%) inpatient studies and in 28/62 (45.2%) outpatient studies. For this measure, we found a median MMR of 3.7 (IQR 2.6-5.0) in 4 studies reporting antibiotic use in ICUs in DDDs/1000 patient-days and a median MMR of 2.3 (IQR 1.5-3.2) in 18 studies reporting outpatient antibiotic use in DDDs/1000 inhabitant-days. Substantial variation was also identified in other measures.
Conclusions: Our review confirms the large variation in antibiotic use even across similar settings and providers. Data from low- and middle-income countries are under-represented. Further studies should try to better elucidate reasons for the observed variation to facilitate interventions that reduce unwarranted practice variation. In addition, the heterogeneity of reported measures clearly shows that there is need for standardization.
References
-
- Harbarth S, Theuretzbacher U, Hackett J.. Antibiotic research and development: business as usual? J Antimicrob Chemother 2015; 70: 1604–7. - PubMed
-
- Wennberg J, Gittelsohn A.. Small area variations in health care delivery. Science 1973; 182: 1102–8. - PubMed
-
- Kuster SP, Rudnick W, Shigayeva A. et al. Previous antibiotic exposure and antimicrobial resistance in invasive pneumococcal disease: results from prospective surveillance. Clin Infect Dis 2014; 59: 944–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
