

Competition for blood flow distribution between respiratory and locomotor muscles: implications for muscle fatigue
- PMID: 29878876
- PMCID: PMC6842878
- DOI: 10.1152/japplphysiol.00189.2018
Competition for blood flow distribution between respiratory and locomotor muscles: implications for muscle fatigue
Abstract
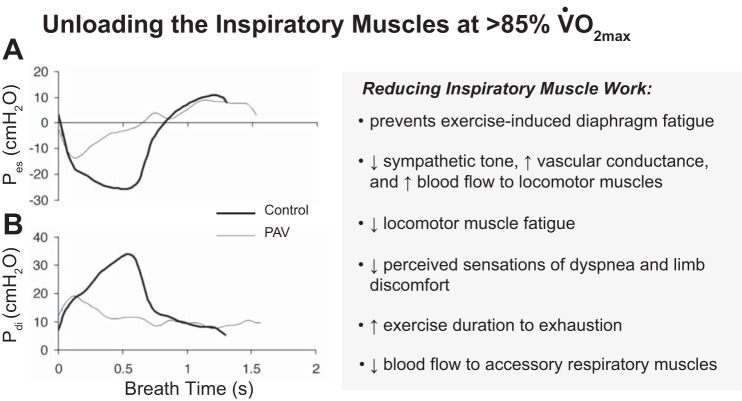
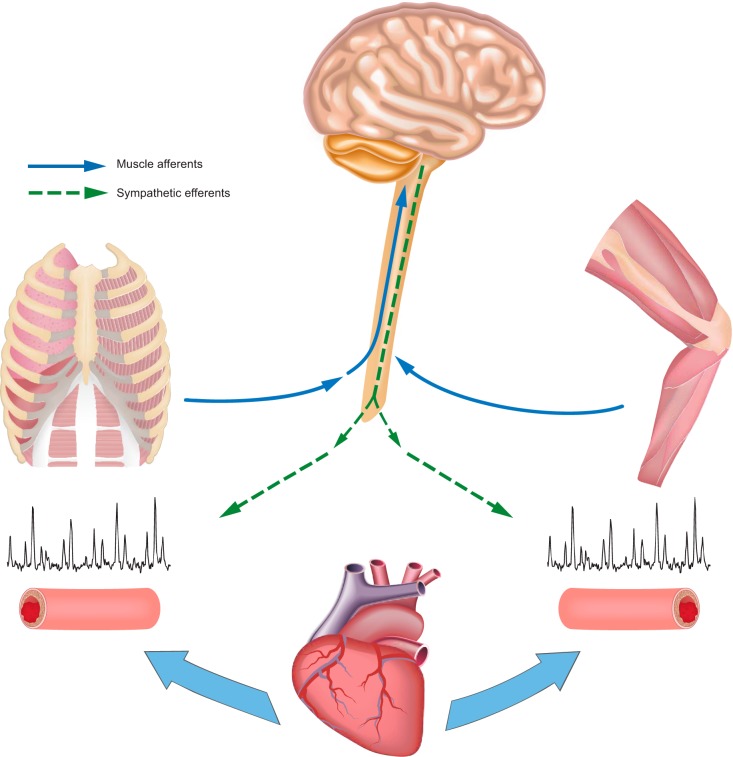
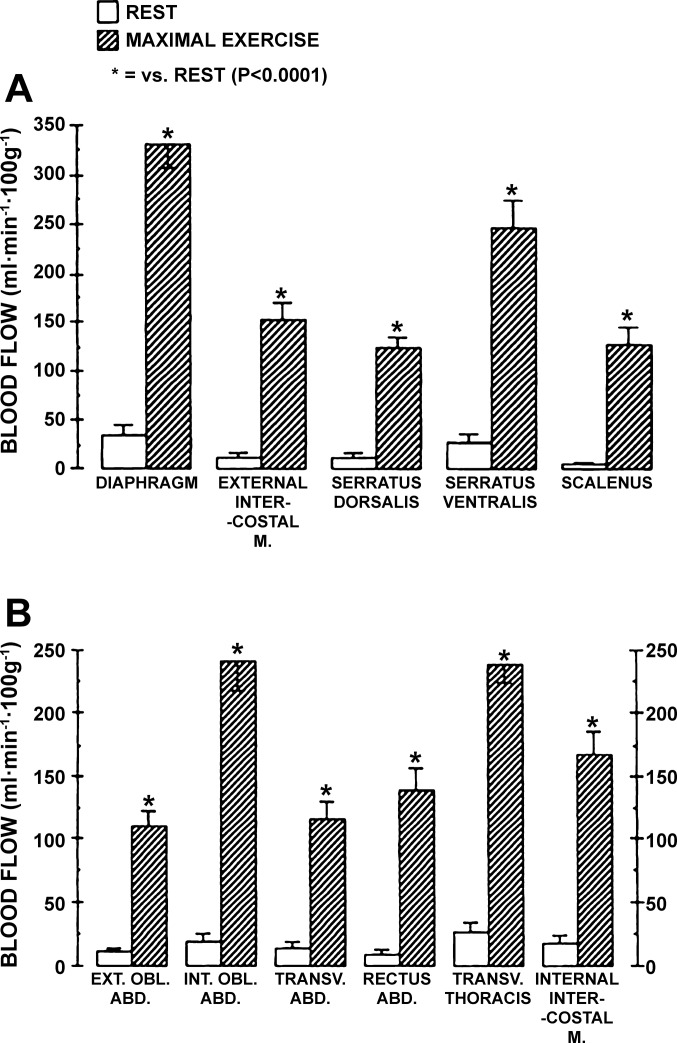
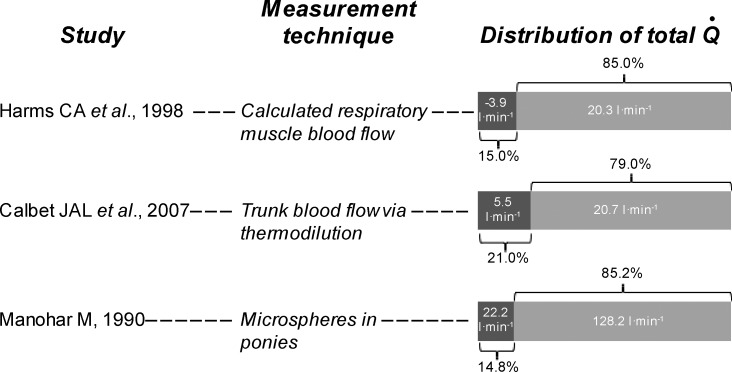
Sympathetically induced vasoconstrictor modulation of local vasodilation occurs in contracting skeletal muscle during exercise to ensure appropriate perfusion of a large active muscle mass and to maintain also arterial blood pressure. In this synthesis, we discuss the contribution of group III-IV muscle afferents to the sympathetic modulation of blood flow distribution to locomotor and respiratory muscles during exercise. This is followed by an examination of the conditions under which diaphragm and locomotor muscle fatigue occur. Emphasis is given to those studies in humans and animal models that experimentally changed respiratory muscle work to evaluate blood flow redistribution and its effects on locomotor muscle fatigue, and conversely, those that evaluated the influence of coincident limb muscle contraction on respiratory muscle blood flow and fatigue. We propose the concept of a "two-way street of sympathetic vasoconstrictor activity" emanating from both limb and respiratory muscle metaboreceptors during exercise, which constrains blood flow and O2 transport thereby promoting fatigue of both sets of muscles. We end with considerations of a hierarchy of blood flow distribution during exercise between respiratory versus locomotor musculatures and the clinical implications of muscle afferent feedback influences on muscle perfusion, fatigue, and exercise tolerance.
Keywords: blood flow; diaphragm; exercise; metaboreflex; sympathetic vasoconstriction; work of breathing.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
Similar articles
-
Respiratory muscle energetics during exercise in healthy subjects and patients with COPD.Respir Med. 2006 Nov;100(11):1896-906. doi: 10.1016/j.rmed.2006.02.030. Epub 2006 May 4. Respir Med. 2006. PMID: 16677807 Review.
-
Effect of increased inspiratory muscle work on blood flow to inactive and active limbs during submaximal dynamic exercise.Exp Physiol. 2019 Feb;104(2):180-188. doi: 10.1113/EP087380. Epub 2018 Dec 9. Exp Physiol. 2019. PMID: 30462876
-
The hyperpnoea of exercise in health: Respiratory influences on neurovascular control.Exp Physiol. 2020 Dec;105(12):1984-1989. doi: 10.1113/EP088103. Epub 2020 Mar 16. Exp Physiol. 2020. PMID: 32034952 Review.
-
Exercise-induced respiratory muscle fatigue: implications for performance.J Appl Physiol (1985). 2008 Mar;104(3):879-88. doi: 10.1152/japplphysiol.01157.2007. Epub 2007 Dec 20. J Appl Physiol (1985). 2008. PMID: 18096752 Review.
-
Consequences of exercise-induced respiratory muscle work.Respir Physiol Neurobiol. 2006 Apr 28;151(2-3):242-50. doi: 10.1016/j.resp.2005.12.015. Respir Physiol Neurobiol. 2006. PMID: 16616716 Review.
Cited by
-
Monitoring Changes in Oxygen Muscle during Exercise with High-Flow Nasal Cannula Using Wearable NIRS Biosensors.Biosensors (Basel). 2023 Nov 13;13(11):985. doi: 10.3390/bios13110985. Biosensors (Basel). 2023. PMID: 37998160 Free PMC article.
-
Ventilatory Limitation of Exercise in Pediatric Subjects Evaluated for Exertional Dyspnea.Front Physiol. 2019 Jan 29;10:20. doi: 10.3389/fphys.2019.00020. eCollection 2019. Front Physiol. 2019. PMID: 30761012 Free PMC article.
-
Unraveling the Role of Respiratory Muscle Metaboloreceptors under Inspiratory Training in Patients with Heart Failure.Int J Environ Res Public Health. 2021 Feb 10;18(4):1697. doi: 10.3390/ijerph18041697. Int J Environ Res Public Health. 2021. PMID: 33578776 Free PMC article. Review.
-
Face Masks and the Cardiorespiratory Response to Physical Activity in Health and Disease.Ann Am Thorac Soc. 2021 Mar;18(3):399-407. doi: 10.1513/AnnalsATS.202008-990CME. Ann Am Thorac Soc. 2021. PMID: 33196294 Free PMC article. Review.
-
Effects of inspiratory muscle training on 1RM performance and body composition in professional natural bodybuilders.Front Physiol. 2025 Apr 7;16:1574439. doi: 10.3389/fphys.2025.1574439. eCollection 2025. Front Physiol. 2025. PMID: 40260203 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources