

Effect of Budesonide Added to Large-Volume, Low-pressure Saline Sinus Irrigation for Chronic Rhinosinusitis: A Randomized Clinical Trial
- PMID: 29879268
- PMCID: PMC6145785
- DOI: 10.1001/jamaoto.2018.0667
Effect of Budesonide Added to Large-Volume, Low-pressure Saline Sinus Irrigation for Chronic Rhinosinusitis: A Randomized Clinical Trial
Abstract
Importance: Recent studies suggest that budesonide added to saline nasal lavage can be an effective treatment for patients with chronic rhinosinusitis (CRS).
Objective: To evaluate the incremental effect of adding budesonide to large-volume, low-pressure saline sinus irrigation.
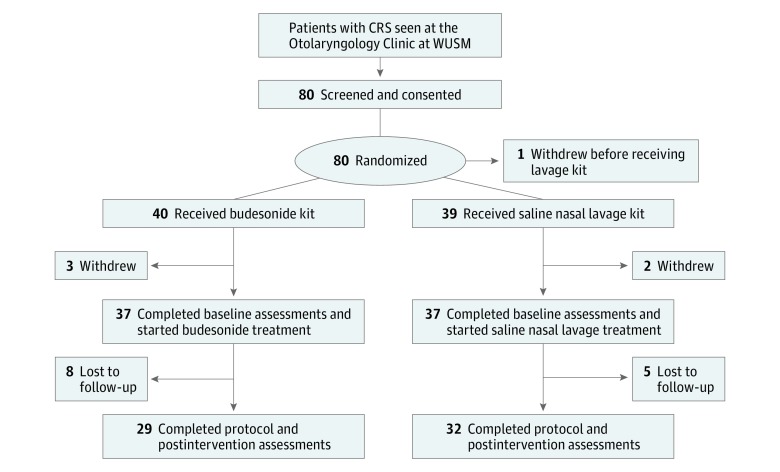
Design, setting, and participants: This double-blind, placebo-controlled, randomized clinical trial was conducted at a quaternary care academic medical center between January 1, 2016, and February 16, 2017. A total of 80 adult patients with CRS were enrolled; 74 completed baseline assessments; and 61 remained in the trial to complete all analyses. Data analysis was conducted from March 2017 to August 2017.
Interventions: All study participants were provided with a sinus rinse kit including saline and identical-appearing capsules that contained either budesonide (treatment group) or lactose (control group). Patients were instructed to dissolve the capsules in the saline and use the resulting solution to irrigate both nasal cavities, using half the solution for each cavity, once daily for 30 days.
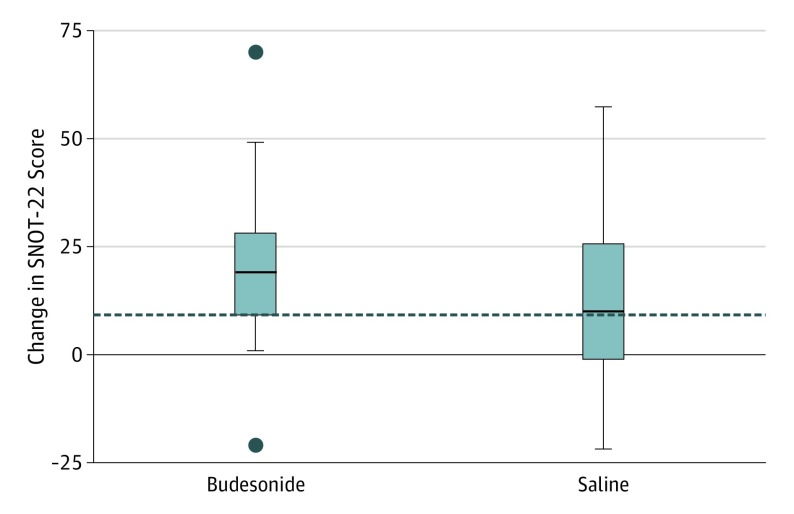
Main outcomes and measures: The primary outcome measure was the change in Sino-Nasal Outcome Test (SNOT-22) scores, pretreatment to posttreatment, in the budesonide group compared with the control group. Secondary outcome measures included patient-reported response to treatment, as measured with a modification of the Clinical Global Impressions scale, and endoscopic examination scored by the Lund-Kennedy grading system.
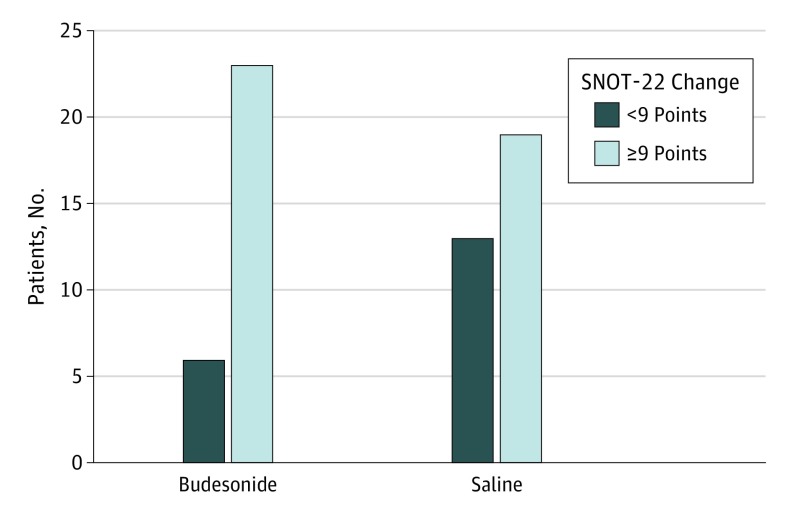
Results: Of the 74 participants who completed baseline assessments (37 in each study arm), mean (SD) age, 51 (14.7) years, 50 (68%) were women. Of the 61 who remained in the trial to complete all analyses, 29 were randomized to budesonide treatment, and 32 to saline alone. The average change in SNOT-22 scores was 20.7 points for those in the budesonide group and 13.6 points for those in the control group, for a mean difference of 7 points in favor of the budesonide group (95% CI, -2 to 16). A total of 23 participants (79%) in the budesonide group experienced a clinically meaningful reduction in their SNOT-22 scores compared with 19 (59%) in the control group, for a difference of 20% (95% CI, -2.5% to 42.5%). The average change in endoscopic scores was 3.4 points for the budesonide group and 2.7 points for the control group. There were no related adverse events.
Conclusions and relevance: This study shows that budesonide in saline nasal lavage results in clinically meaningful benefits beyond the benefits of saline alone for patients with CRS. Given the imprecision in the treatment effect, further research is warranted to define the true effect of budesonide in saline nasal lavage.
Trial registration: ClinicalTrials.gov Identifier: NCT02696850.
Conflict of interest statement
Figures
Comment in
-
Building the Evidence for Corticosteroid Irrigation Therapy in Chronic Rhinosinusitis.JAMA Otolaryngol Head Neck Surg. 2018 Jul 1;144(7):612-613. doi: 10.1001/jamaoto.2018.0642. JAMA Otolaryngol Head Neck Surg. 2018. PMID: 29879273 No abstract available.
References
-
- Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. . Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2)(suppl):S1-S39. - PubMed
-
- Ray NF, Baraniuk JN, Thamer M, et al. . Healthcare expenditures for sinusitis in 1996: contributions of asthma, rhinitis, and other airway disorders. J Allergy Clin Immunol. 1999;103(3 Pt 1):408-414. - PubMed
-
- Bhattacharyya N. Incremental healthcare utilization and expenditures for allergic rhinitis in the United States. Laryngoscope. 2011;121(9):1830-1833. - PubMed
-
- Dass K, Peters AT. Diagnosis and Management of Rhinosinusitis: Highlights from the 2015 Practice Parameter. Curr Allergy Asthma Rep. 2016;16(4):29. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, et al. . EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1)(suppl 23):1-12. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
