

Incidence of Diabetes After Cancer Development: A Korean National Cohort Study
- PMID: 29879271
- PMCID: PMC6143049
- DOI: 10.1001/jamaoncol.2018.1684
Incidence of Diabetes After Cancer Development: A Korean National Cohort Study
Abstract
Importance: Diabetes is an established risk factor for developing cancer. A limited body of evidence also suggests that cancer can increase the risk of developing new cases of diabetes, but the evidence is inconclusive.
Objective: To evaluate whether the development of cancer is associated with increasing risk of subsequent diabetes.
Design, setting, and participants: This cohort study included a nationally representative sample of the Korean general population observed for up to 10 years (January 1, 2003, to December 31, 2013). A total of 524 089 men and women 20 to 70 years of age without diabetes and with no history of cancer at baseline were included.
Exposures: Incident cancer (time-varying exposure).
Main outcomes and measures: Incident type 2 diabetes using insurance claim codes.
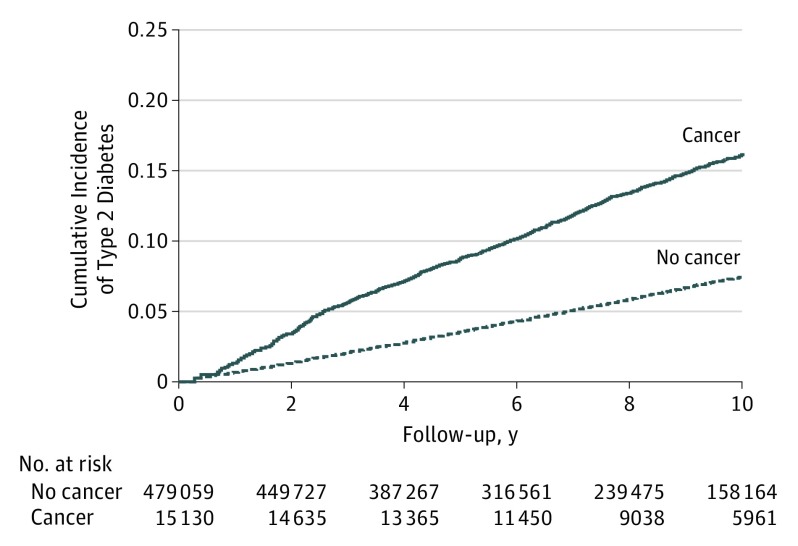
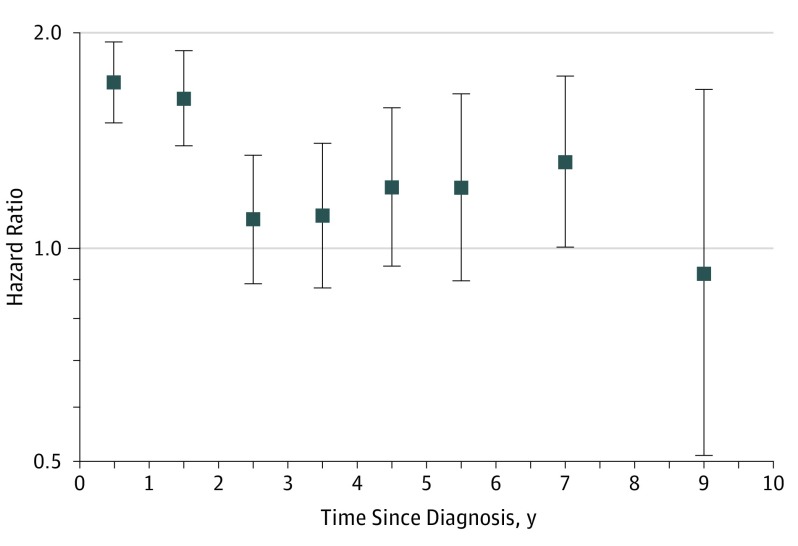
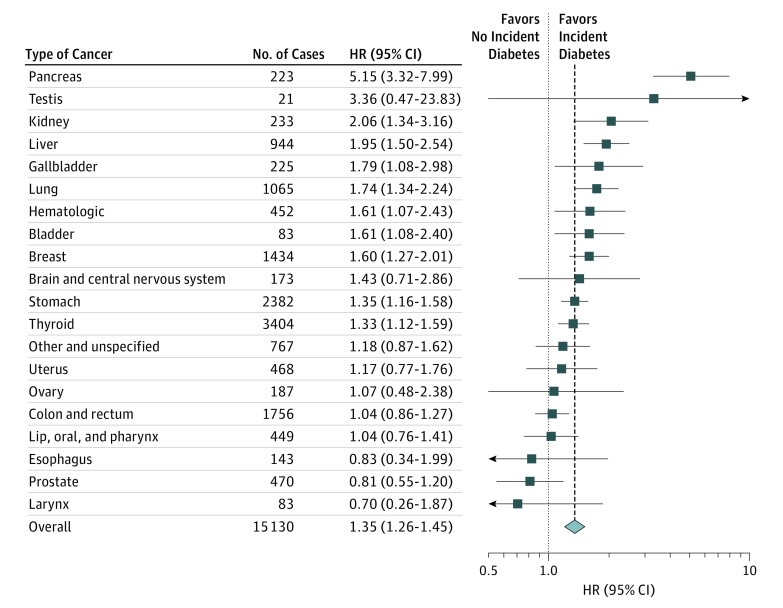
Results: During 3 492 935.6 person-years of follow-up (median follow-up, 7.0 years) in 494 189 individuals (50.0% female; mean [SD] age, 41.8 [12.5] years), 15 130 participants developed cancer and 26 610 participants developed diabetes. After adjustment for age, sex, precancer diabetes risk factors, metabolic factors, and comorbidities, the hazard ratio (HR) for diabetes associated with cancer development was 1.35 (95% CI, 1.26-1.45; P < .001). The excess risk for diabetes was highest in the first 2 years after cancer diagnosis, but it remained elevated throughout follow-up. By cancer type, development of pancreatic (HR, 5.15; 95% CI, 3.32-7.99), kidney (HR, 2.06; 95% CI, 1.34-3.16), liver (HR, 1.95; 95% CI, 1.50-2.54), gallbladder (HR, 1.79; 95% CI, 1.08-2.98), lung (HR, 1.74; 95% CI, 1.34-2.24), blood (HR, 1.61; 95% CI, 1.07-2.43), breast (HR, 1.60; 95% CI, 1.27-2.01), stomach (HR, 1.35; 95% CI, 1.16-1.58), and thyroid cancer (HR, 1.33; 95% CI, 1.12-1.59) was associated with a significantly increased risk of diabetes.
Conclusions and relevance: In this large Korean cohort, cancer development increased the risk of subsequent diabetes. These data provide evidence that cancer is associated with an increased risk of diabetes in cancer survivors independent of traditional diabetes risk factors. Physicians should remember that patients with cancer develop other clinical problems, such as diabetes, with higher frequency than individuals without cancer, and should consider routine diabetes screening in these patients.
Conflict of interest statement
Figures
Comment in
-
Risk of Diabetes Associated With Cancer Development.JAMA Oncol. 2019 Mar 1;5(3):429. doi: 10.1001/jamaoncol.2018.6619. JAMA Oncol. 2019. PMID: 30653207 No abstract available.
-
Risk of Diabetes Associated With Cancer Development-In Reply.JAMA Oncol. 2019 Mar 1;5(3):429-430. doi: 10.1001/jamaoncol.2018.6647. JAMA Oncol. 2019. PMID: 30653218 No abstract available.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-E386. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7-30. - PubMed
-
- Holmes HM, Nguyen HT, Nayak P, Oh JH, Escalante CP, Elting LS. Chronic conditions and health status in older cancer survivors. Eur J Intern Med. 2014;25(4):374-378. - PubMed
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747-1757. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
